Activity
Mon
Wed
Fri
Sun
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
What is this?
Less
More
Owned by Leanna
Free wellness community for faith based living, functional health and real connection - off social media, rooted in purpose - learn, grow and heal.
Memberships
Skoolers
165.6k members • Free
219 contributions to Bedrock Nation

17d •
Why My Pulsetto Vagus Nerve Stimulator Is One of My Favorite Health Tools
How I use it for stress, anxiety, burnout, recovery, gut health, and nervous system regulation. If you’ve been around Bedrock Nutrition for any length of time, you’ve probably heard me say that symptoms are often the body’s way of communicating—not the problem itself. Anxiety. Digestive issues. Poor sleep. Chronic pain. Fatigue. Burnout. Many times, these aren’t isolated problems. They’re signs that the nervous system is struggling to adapt. That’s why one of my favorite tools over the past year has been my Pulsetto vagus nerve stimulator. I use it regularly myself, recommend it to many clients, and consider it one of the most practical ways to support the body’s built-in healing system. First: What Is the Vagus Nerve? The vagus nerve is the longest cranial nerve in the body. It connects the brain to many of your most important organs, including: - Heart - Lungs - Digestive tract - Liver - Pancreas - Spleen Think of it as the body’s primary communication highway. It helps regulate: - Stress response - Heart rate - Digestion - Inflammation - Mood - Sleep - Recovery When vagal tone is strong, the body is better able to move into a parasympathetic state—often called “rest, digest, heal, and recover.” When vagal tone is poor, people often feel stuck in survival mode. The Problem: Most People Are Living in Fight-or-Flight The modern world keeps the nervous system constantly stimulated. Emails. News. Social media. Financial pressure. Family stress. Lack of sleep. Inflammation. Poor nutrition. The body interprets all of these as stressors. Over time, people begin experiencing symptoms such as: - Anxiety - Panic feelings - Racing thoughts - Digestive problems - IBS - Poor sleep - Fatigue - Increased pain - Hormonal imbalances - Brain fog - Burnout

0 likes • 15d
@Kirsten Doehle i’m so glad to hear your feedback!
17d •
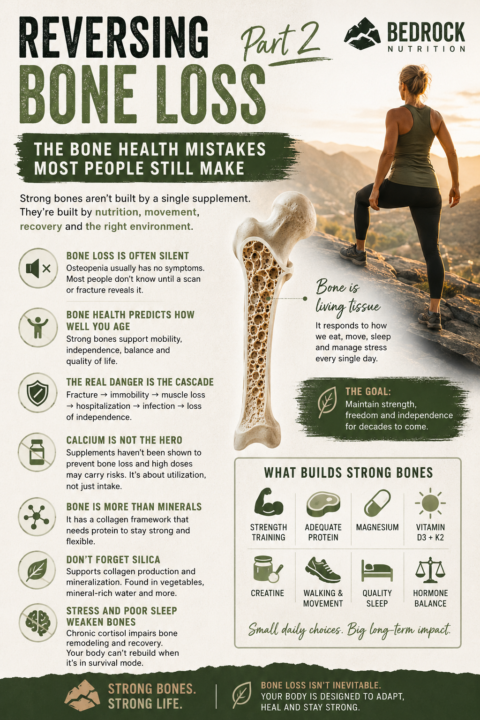
Reversing Bone Loss Part 2: The Bone Health Mistakes Most People Still Make
The Bone Health Mistakes Most People Still Make After publishing my recent article on reversing bone loss, I realized there were several important concepts that deserved their own discussion. Most people understand that bones need nutrients. What many don’t realize is that bone loss is often a symptom of deeper dysfunction occurring elsewhere in the body. If you’ve been diagnosed with osteopenia or osteoporosis, these additional factors may be just as important as the supplements you’re taking. 1. Bone Loss Is Often Silent One of the most dangerous things about osteopenia is that most people don’t know they have it. There is usually no pain. No warning sign. No obvious symptom. In many cases, the first indication something is wrong is a bone density scan or an unexpected fracture. This is why I often remind clients: The absence of symptoms does not mean the absence of disease. Bone loss can be occurring for years before it becomes obvious. 2. Bone Health Predicts How Well We Age When most people think about osteoporosis, they think about broken bones. But bone health is about much more than fractures. Strong bones are closely linked to: - Independence - Mobility - Balance - Strength - Fall prevention - Recovery from illness - Overall longevity The ability to get off the floor, climb stairs, carry groceries, travel, and remain active later in life often depends on maintaining both muscle mass and bone density. Bone health is really a quality-of-life issue. 3. The Real Danger Isn’t the Fracture There is an old saying in medicine: “Break your hip, die of pneumonia.” While that may sound dramatic, it highlights an important reality. The fracture itself is often not the greatest danger. The real threat is what happens afterward. Fracture. Hospitalization. Surgery. Immobility. Muscle loss. Loss of independence.
1
0
17d •
Reversing Bone Loss: What Actually Builds Strong Bones?
When most people hear the words osteopenia or osteoporosis, they immediately think: “I need more calcium.” But the truth is that bone health is far more complicated than simply taking a calcium supplement. Bone is living tissue. It is constantly being broken down and rebuilt. If we want to improve bone density, we have to create an environment where the body can build new bone faster than it loses it. Here are some of the most important factors I focus on when helping clients support healthy bones. 1. Adequate Protein: The Foundation of Bone Many people don’t realize that bone is approximately 50% protein by volume. Without adequate protein, your body simply does not have the raw materials needed to rebuild and maintain strong bones. Protein also supports: - Muscle mass - Balance and stability - Reduced fall risk - Recovery from exercise Most adults, especially those over 40, need significantly more protein than they are currently consuming. Goal: Prioritize a protein-forward diet at every meal. 2. Magnesium: The Mineral Most People Are Missing Magnesium is involved in hundreds of biochemical processes, including bone formation. Low magnesium can contribute to: - Poor vitamin D utilization - Muscle weakness - Increased inflammation - Impaired bone remodeling Unfortunately, modern soils are depleted, stress burns through magnesium rapidly, and many adults are deficient. Goal: Prioritize magnesium-rich foods and consider supplementation when appropriate. 3. Vitamin D3 and K2: The Dynamic Duo Vitamin D helps increase calcium absorption. Vitamin K2 helps direct that calcium where it belongs—into bones and teeth rather than soft tissues. I rarely recommend D3 without K2 because they work together. Optimal vitamin D levels are often significantly higher than the minimum “normal” range reported on lab work. Goal: Maintain healthy vitamin D levels while ensuring adequate K2 intake. 4. Creatine: Not Just for Athletes (IDL LOAD) Creatine is one of the most researched supplements in the world.
2
0
23d •
Why You Can’t Sleep:
A Terrain-Based Approach to Insomnia and Sleep Disturbances Most people think insomnia is a sleep problem. I don’t. Insomnia is often a symptom of an underlying imbalance. The inability to fall asleep, stay asleep, or wake feeling restored is rarely caused by a deficiency of sleeping pills. More often, it is the result of dysfunction somewhere upstream. The body is designed to sleep. When it doesn’t, something is interfering with that design. Instead of asking: “What can I take to make me sleep?” A better question is: “Why does my body no longer feel safe enough to sleep?” Sleep Is Not Passive Many people think of sleep as a period when the body shuts down. In reality, sleep is one of the most active healing states in human physiology. During sleep, your body: - Repairs tissues - Produces growth hormone - Consolidates memories - Regulates blood sugar - Balances hormones - Clears metabolic waste from the brain - Supports immune function - Repairs cellular damage Sleep is not a luxury. It’s a biological requirement. When sleep becomes disrupted, every system in the body eventually suffers. The Four Most Common Root Causes of Insomnia 1. Stress and Elevated Cortisol This is by far the most common cause I see. Your body cannot simultaneously prepare for survival and prepare for sleep. When cortisol remains elevated into the evening, the brain receives a message: “Stay alert. We may need to deal with a threat.” The result: - Difficulty falling asleep - Racing thoughts - Waking between 1–4 AM - Light, non-restorative sleep - Feeling tired but wired Many people assume they have a sleep problem when what they actually have is a stress regulation problem. Research consistently shows that people with insomnia often exhibit higher nighttime cortisol levels and a state of physiologic hyperarousal. 2. Blood Sugar Dysregulation This is another commonly overlooked cause. Blood sugar instability during the night can trigger: - Adrenaline release - Cortisol release - Night sweats - Racing heart - Sudden awakening around 2–4 AM
4
0

24d •
The Real Reason We Can't Stop Scrolling
Hint: It's Not Dopamine. If you've spent any time on social media lately, you've probably heard people talk about "dopamine addiction." Dopamine detoxes. Dopamine overload. Dopamine fasting. Dopamine being the reason we can't put our phones down. But what if dopamine isn't the problem? What if we're blaming one of the body's most important systems for a problem it never created? Dopamine isn't bad. In fact, dopamine is one of the most remarkable systems God designed into the human body. Without dopamine: • You wouldn't pursue goals. • You wouldn't feel motivated. • You wouldn't experience anticipation. • You wouldn't enjoy learning. • You wouldn't strive for improvement. • You wouldn't seek meaningful connection. Dopamine is part of the system that helps move us forward. It was designed to reward behaviors that help us survive, grow, learn, connect, and fulfill our purpose. So if dopamine isn't the problem... Why can't we stop scrolling? Because modern life has learned how to trigger the reward without requiring the growth. For most of human history, dopamine was tied to effort. You learned a skill. You built something. You solved a problem. You worked toward a goal. You spent time with people you loved. You served others. You deepened your faith. You accomplished something meaningful. And dopamine reinforced those behaviors. Today, we can access the reward without the process. A notification. A like. A comment. A reel. A short video. A purchase. A swipe. A scroll. The brain receives a reward signal, but often without the growth, purpose, or fulfillment that was originally meant to accompany it. Over time, that disconnect can create imbalance. But I think there's an even deeper question worth asking. Why do some people scroll for ten minutes and put the phone down... While others lose three hours? Why can one person enjoy social media without becoming dependent... While another feels compelled to check every notification? The answer is usually much bigger than dopamine.

1-10 of 219

@leanna-cappucci-3527
Functional Nutritionist, Mother, Free Thinker, Christian, Writer/Educator
Active 4d ago
Joined Nov 4, 2025
INTJ
Florida, USA