
Write something

13d •
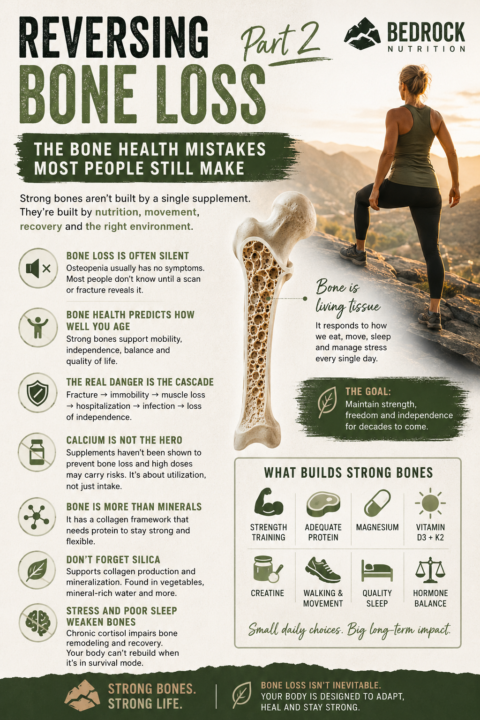
Reversing Bone Loss Part 2: The Bone Health Mistakes Most People Still Make
The Bone Health Mistakes Most People Still Make After publishing my recent article on reversing bone loss, I realized there were several important concepts that deserved their own discussion. Most people understand that bones need nutrients. What many don’t realize is that bone loss is often a symptom of deeper dysfunction occurring elsewhere in the body. If you’ve been diagnosed with osteopenia or osteoporosis, these additional factors may be just as important as the supplements you’re taking. 1. Bone Loss Is Often Silent One of the most dangerous things about osteopenia is that most people don’t know they have it. There is usually no pain. No warning sign. No obvious symptom. In many cases, the first indication something is wrong is a bone density scan or an unexpected fracture. This is why I often remind clients: The absence of symptoms does not mean the absence of disease. Bone loss can be occurring for years before it becomes obvious. 2. Bone Health Predicts How Well We Age When most people think about osteoporosis, they think about broken bones. But bone health is about much more than fractures. Strong bones are closely linked to: - Independence - Mobility - Balance - Strength - Fall prevention - Recovery from illness - Overall longevity The ability to get off the floor, climb stairs, carry groceries, travel, and remain active later in life often depends on maintaining both muscle mass and bone density. Bone health is really a quality-of-life issue. 3. The Real Danger Isn’t the Fracture There is an old saying in medicine: “Break your hip, die of pneumonia.” While that may sound dramatic, it highlights an important reality. The fracture itself is often not the greatest danger. The real threat is what happens afterward. Fracture. Hospitalization. Surgery. Immobility. Muscle loss. Loss of independence.
1
0
14d •
Reversing Bone Loss: What Actually Builds Strong Bones?
When most people hear the words osteopenia or osteoporosis, they immediately think: “I need more calcium.” But the truth is that bone health is far more complicated than simply taking a calcium supplement. Bone is living tissue. It is constantly being broken down and rebuilt. If we want to improve bone density, we have to create an environment where the body can build new bone faster than it loses it. Here are some of the most important factors I focus on when helping clients support healthy bones. 1. Adequate Protein: The Foundation of Bone Many people don’t realize that bone is approximately 50% protein by volume. Without adequate protein, your body simply does not have the raw materials needed to rebuild and maintain strong bones. Protein also supports: - Muscle mass - Balance and stability - Reduced fall risk - Recovery from exercise Most adults, especially those over 40, need significantly more protein than they are currently consuming. Goal: Prioritize a protein-forward diet at every meal. 2. Magnesium: The Mineral Most People Are Missing Magnesium is involved in hundreds of biochemical processes, including bone formation. Low magnesium can contribute to: - Poor vitamin D utilization - Muscle weakness - Increased inflammation - Impaired bone remodeling Unfortunately, modern soils are depleted, stress burns through magnesium rapidly, and many adults are deficient. Goal: Prioritize magnesium-rich foods and consider supplementation when appropriate. 3. Vitamin D3 and K2: The Dynamic Duo Vitamin D helps increase calcium absorption. Vitamin K2 helps direct that calcium where it belongs—into bones and teeth rather than soft tissues. I rarely recommend D3 without K2 because they work together. Optimal vitamin D levels are often significantly higher than the minimum “normal” range reported on lab work. Goal: Maintain healthy vitamin D levels while ensuring adequate K2 intake. 4. Creatine: Not Just for Athletes (IDL LOAD) Creatine is one of the most researched supplements in the world.
2
0
21d •
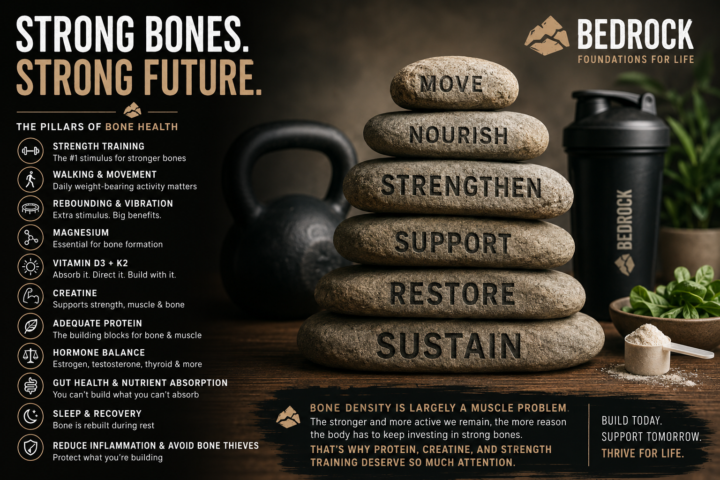
How We Build a Supplement Plan at Bedrock
After reading the first three parts of this series, some people might be wondering: "If vitamins don't work alone, nutrients work in teams, and more supplements aren't always better... then how do I know what I should take?" It's a fair question. And the answer is probably not what most supplement companies want you to hear. We don't start with supplements. We start with foundations. Because no supplement can consistently overcome poor foundations. If someone is sleeping 4-5 hours per night, eating ultra-processed food, dehydrated, sedentary, stressed, and disconnected from sunlight, the solution is rarely another capsule. The body is asking for something much deeper. At Bedrock, we focus on what I call the terrain. T he environment in which every cell, hormone, nutrient, enzyme, and organ system must function. When the terrain improves, health often improves. When the terrain deteriorates, symptoms begin to appear. That's why we focus on our Seven Pillars: ✓ Food ✓ Supplements ✓ Hydration ✓ Sunlight ✓ Sleep ✓ Movement ✓ Stress & Spiritual Health Most people want to jump straight to supplements. But supplements are only one pillar. Not the foundation. Not the entire structure. Just one tool. Once the foundations are in place, we begin asking better questions. What is the body actually communicating? What symptoms are present? What systems appear stressed? What nutrient relationships may be struggling? Where are the bottlenecks? This is why we often recommend testing before guessing. A symptom doesn't automatically tell us what nutrient is missing. Fatigue isn't always iron. Brain fog isn't always B12. Poor sleep isn't always melatonin. Low energy isn't always caffeine. The body speaks in patterns. Our job is to learn the language. When we do recommend supplements, we look for leverage. We aren't trying to create the largest supplement stack possible. We're looking for the smallest intervention that produces the greatest improvement. We focus on:
2
0

21d •
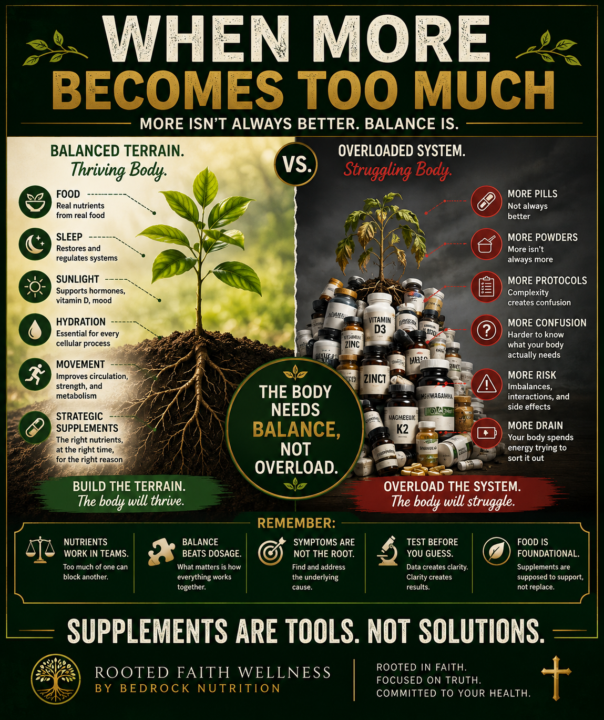
Why More Supplements Can Make Things Worse
In Part 1, we talked about the biggest lie about vitamins: Nutrients don't work alone. In Part 2, we talked about why nutrients work in teams. Today, let's talk about one of the most common mistakes I see in health and wellness: The belief that more supplements automatically create better health. Unfortunately, that's not how biology works. In fact, sometimes the exact opposite is true. Most people approach supplements like they're trying to fill a bucket. Low energy? Add B vitamins. Trouble sleeping? Add melatonin. Low Vitamin D? Take more D. Hair loss? Add biotin. Joint pain? Add collagen. Then they add another supplement. And another. And another. Before long, they have a cabinet full of products and no real understanding of what their body actually needs. The problem is that the body isn't a bucket. It's an ecosystem. And ecosystems depend on balance. Take Vitamin D as an example. Many people know they need Vitamin D. So they start taking 5,000, 10,000, or even 20,000 IU per day. But Vitamin D requires magnesium for activation. It works alongside Vitamin K2. It influences calcium metabolism. It affects multiple hormone pathways. When you push one nutrient aggressively without supporting the others, you can create new imbalances. The same thing happens with calcium. For years, people were told: "Take calcium for strong bones." So they did. Millions of people added calcium supplements without addressing: • Vitamin D3 • Vitamin K2 • Magnesium • Stomach acid • Hormonal health The result? More calcium wasn't necessarily building stronger bones. In many cases it was simply increasing the amount of calcium circulating in the body. Leading to kidney stones, gallstones, joint pain, arterial calcification... but not "stronger bones." As a matter of fact, with the underlying problem not addressed, bone loss can even get worse... Iron is another example. People feel tired. They assume they're low in iron. They start supplementing. But excess iron can increase oxidative stress and inflammation.
1
0
21d •
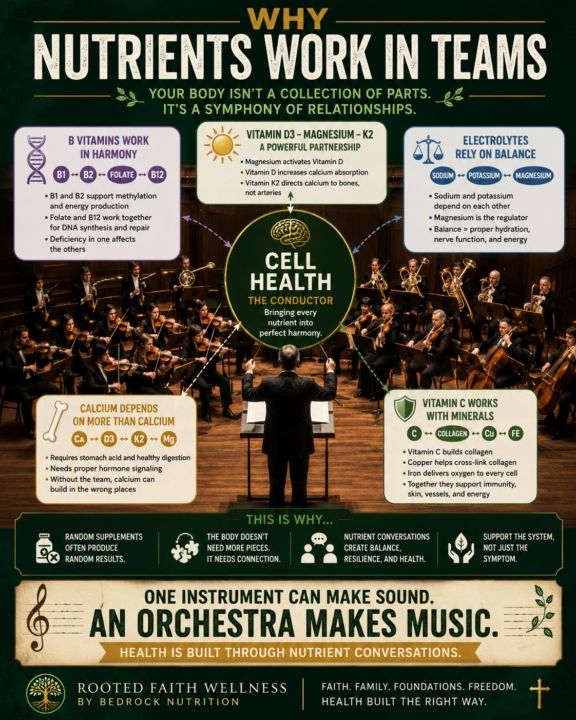
Why Nutrients Work in Teams
In Part 1, we talked about the biggest lie we've been told about vitamins: That nutrients work independently. They don't. Today, let's talk about why. Imagine trying to build a house. You have lumber. But no nails. Or nails, but no hammer. Or a hammer, but no foundation. Every piece has value, but none of them can complete the project alone. Your body works the same way. Every vitamin, mineral, amino acid, enzyme, and hormone participates in an intricate network of biochemical relationships. This is why I often say: The body doesn't run on nutrients.The body runs on nutrient conversations. Take Vitamin D, for example. Most people know Vitamin D is important. What most people don't realize is that Vitamin D isn't even fully active until magnesium helps convert it into its usable form. Then Vitamin K2 helps direct calcium into bones and teeth instead of allowing it to accumulate in soft tissues and arteries. Without magnesium? The conversation breaks down. Without K2? The conversation breaks down. Vitamin D isn't working alone. Neither are they. The same thing happens with the B vitamins. Many people think of B12 as the "energy vitamin." But B12 doesn't work by itself. B1 and B2 support important pathways involved in methylation and energy production. Folate and B12 work together. Deficiency in one can create problems that appear to be caused by another. This is one reason isolated supplementation sometimes fails. The body was expecting a team. We gave it a single player. Minerals operate the same way. Potassium depends on sodium. Sodium depends on potassium. Both rely heavily on magnesium. When one becomes excessive or deficient, the entire system shifts. That's why simply taking more potassium isn't always the answer. The body is constantly balancing relationships. Calcium is another perfect example. For decades we've been told: "Take calcium for strong bones." But calcium doesn't build healthy bones by itself. Calcium requires: • Vitamin D3• Vitamin K2• Magnesium• Adequate stomach acid• Healthy digestion• Proper hormone signaling
3
0
1-30 of 49
powered by
skool.com/bedrock-nation-8489
Free wellness community for faith based living, functional health and real connection - off social media, rooted in purpose - learn, grow and heal.
Suggested communities
Powered by