
Write something


🔥
2d •
Peptides and Pets: Let's Talk About It 🐾
As always, this is strictly for research and educational purposes — not medical or veterinary advice. If you're considering anything for your pet, please consult with your vet first. You've probably seen this topic floating around, and I think it's time we have an open conversation about it. This little cutie below is my dog Missy, back home in New York. She doesn't look it, but in that second picture, she's 14 years old now. I grew up with this dog. She's family. Missy's been dealing with arthritis for about a year, and it's gotten to the point where she can hardly walk — even with arthritis medication. If you've ever watched a dog you love struggle just to get up and move around, you know how gut-wrenching that is. I've been hesitant to try any peptide protocol with her. This isn't a decision I take lightly. But quality of life is the priority now, and I've seen enough people use BPC-157 and TB-500 with their animals that I think it's time to seriously look into it. So what do these peptides actually do? BPC-157 is a peptide originally derived from a protein in gastric juice. It's been studied in animal models for decades. In simple terms, it helps the body repair itself. It promotes new blood vessel growth around damaged tissue, reduces inflammation through nitric oxide pathways, and has been shown in animal studies to accelerate healing in tendons, ligaments, and muscles — all the things that break down with chronic arthritis. TB-500 is a synthetic version of Thymosin Beta-4, a peptide found naturally in nearly all animal cells. It works by promoting cell migration to injury sites and reducing inflammation. Think of it as the body's way of directing its own repair crew to where it's needed most. It's actually been used in horse medicine for years to treat joint issues and soft tissue injuries, so there's real precedent for animal use. Why use them together? They work through different but complementary pathways. BPC focuses on localized tissue repair and protection, while TB-500 works more systemically through anti-inflammatory and cell repair mechanisms. Together, they attack joint degradation from multiple angles.

🔥
11h •
How to Start Glutathione Without Feeling Like Garbage
Disclaimer: This post is for research and educational purposes only. This is not medical advice. Always consult with a qualified healthcare professional before starting any new protocol. Most people who start researching with glutathione make the same mistake I did: they go too high, too fast, and end up feeling like they got hit by a truck. I'm talking full-on flu-like symptoms. Headaches. Body aches. Fatigue. Brain fog. Nausea. Chills. The whole deal. And then they think glutathione is "bad" or that they're having an allergic reaction, so they stop completely. That's the mistake. They didn't have a bad reaction to glutathione — they just overwhelmed their body's ability to process what glutathione was doing. Let me explain what's actually happening, and then I'll give you the exact protocol I'd follow if I were starting from scratch. So What IS Glutathione? Think of glutathione as your body's master cleanup crew. It's a tiny molecule made up of three amino acids (cysteine, glycine, and glutamate), and it lives in every single cell in your body — with the highest concentration in your liver. Its main jobs: - Neutralizing free radicals (these are unstable molecules that damage your cells — think of them like rust forming on metal) - Detoxifying your liver (it literally grabs onto toxins and heavy metals and makes them water-soluble so your body can flush them out) - Supporting your immune system (it keeps your white blood cells functioning properly) Your body makes glutathione naturally, but as you age, deal with stress, eat poorly, or get exposed to environmental junk, your levels drop. That's where supplementation comes in. Why You Feel Like Garbage When You Start Too High Here's where it gets important. When you introduce a large amount of glutathione into your system all at once, it goes to work immediately — grabbing toxins, heavy metals, and metabolic waste that your body has been storing. The problem? Your body can only eliminate toxins at a certain speed.

🔥
10d •
🧠 Southern Aminos "Neuroluxe" 48mg Blend — Beginner Breakdown
If you've been curious about nootropic (brain-boosting) peptides but feel overwhelmed by the science, this one's for you. Southern Aminos put together a blend called Neuroluxe that targets your brain from four different angles. Let me break down each ingredient in plain English so you actually understand what's going on under the hood. All of this info is for Research and Educational Purposes Only. Not Medical Advice! — What's In It? Pinealon — 11.82 mg → Brain cell protector & sleep support N-Acetyl Selank Amidate — 8.01 mg → Anti-anxiety & calm focus N-Acetyl Semax Amidate — 19.77 mg → Cognitive performance & mental sharpness PE-22-28 — 10.69 mg → Mood support & new brain cell growth Now let's go deeper on each one. 👇 — 1. Pinealon — 11.82 mg Think of it as: Your brain's bodyguard Pinealon is a tiny peptide (only 3 amino acids) originally developed in Russia as a "bioregulator" — basically something that helps restore normal function to a specific tissue. In this case, it targets the central nervous system. What it does: - Protects brain cells from damage. It reduces something called "oxidative stress" — think of oxidative stress as rust building up on your brain cells over time. Pinealon helps prevent that rust. - Reduces cell death. It works on a pathway involving an enzyme called caspase-3, which is basically your cell's self-destruct button. Pinealon helps keep that button from getting pressed unnecessarily. - Supports sleep quality. It works on the pineal gland (the part of your brain that makes melatonin), which may help normalize your sleep-wake cycle. - May support serotonin production. Research suggests it can influence the enzyme (5-tryptophan hydroxylase) that helps your brain make serotonin — your "feel good" neurotransmitter. What makes it unique: Unlike most peptides that work by attaching to receptors on the outside of cells, Pinealon is so small it can actually slip through cell membranes and interact directly with your DNA to influence gene expression. It's working at a deeper level than most compounds.

🔥
Jan 11 •
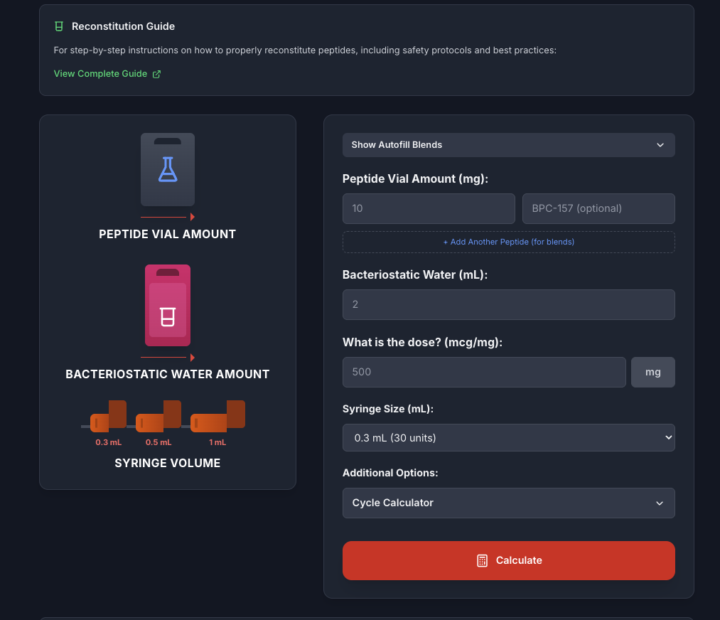
How to Reconstitute Any Peptide Answered
I get questions about reconstitution and research dosing constantly, so here's everything you need to know in one place. I'm building out a comprehensive FAQs section in the Classroom to answer all the common questions I get. If you're still confused after reading this, head over to the Reconstitution FAQ here: https://www.skool.com/peptide-price-9771/classroom/b7dcc989?md=5ef850cf36f5467b9fbb9811f9b69cbf The Most Important Thing to Understand The amount of BAC water you use is entirely up to you. There is no single "correct" amount—you're just choosing how concentrated you want the peptide to be. That said, there are practical guidelines that make the process much easier. My Simple Rule of Thumb (for peptides under 30mg) For every 1 mg of peptide, use 10 units of BAC water. Example with a single peptide: - 20 mg peptide - 10 units per mg - 20 × 10 = 200 units - 200 units = 2 mL of BAC water So you'd reconstitute a 20 mg vial with 2 mL of BAC water. Important Vial Size Rule For anything in a small vial that's over 30 mg, always use 3 mL of BAC water. That's simply the most that will fit in a standard small peptide vial. Once you go past 30 mg, you're no longer choosing concentration freely—you're limited by physical vial volume. What About Blends? For blends, add up the total peptide amount first, then apply the same logic. Example with a blend: - 10 mg BPC-157 - 10 mg TB-500 - Total peptide = 20 mg Now apply the rule: - 20 mg × 10 units = 200 units - 200 units = 2 mL BAC water Blends are reconstituted based on total mg, not each peptide individually. If the total blend exceeds 30 mg in a small vial, use 3 mL. Make It Even Easier With the Calculator I built a calculator specifically for this: https://peptideprice.store/calculator How to use it for a single peptide: 1. Enter Peptide Vial Amount (mg) 2. Enter BAC Water amount (mL) 3. Enter your desired dose 4. Select syringe size 5. Hit Calculate
1-30 of 848
powered by

skool.com/peptide-price-9771
Premier peptide education hub. FREE courses on research peptides & GLP-1s. US supplier intel, safety protocols & expert community support. 🧬🚀
Suggested communities
Powered by