
Write something

May 26 •
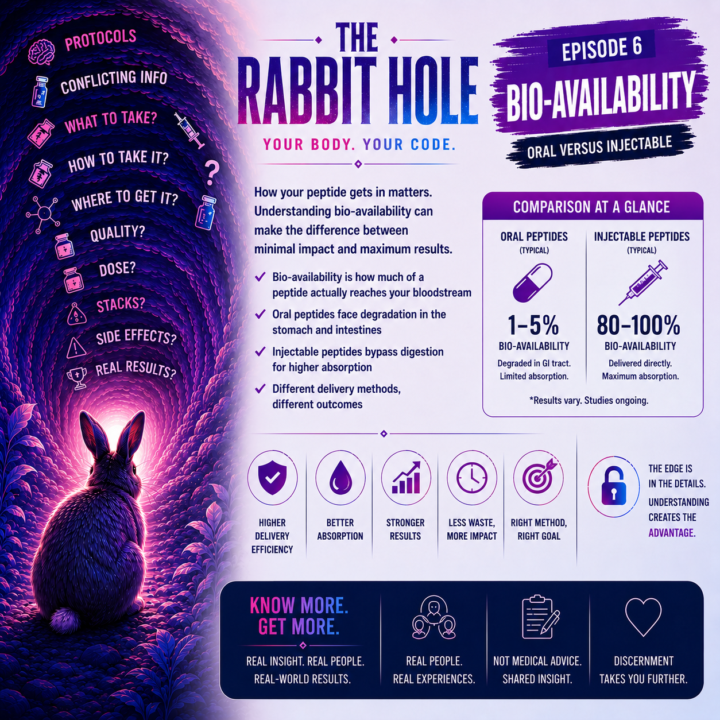
They Call it the Rabbit Hole - Episode #6
A while back we had a discussion around where peptide delivery methods may be heading over the next several years: • capsules • tablets • sublingual delivery • liposomal systems • nasal sprays • transdermal options • and lower-friction administration overall. One of the more interesting parts of this entire discussion is that oral tablets and capsules became the “normal” option long before most people ever started questioning whether they were actually the most efficient delivery method biologically. But honestly, that “normal” likely evolved for a lot of practical reasons:• easier mass production• longer shelf stability• easier transportation and storage• lower manufacturing costs• easier patient compliance• and much broader consumer acceptance. And realistically, a huge percentage of the population simply does not want to deal with injections at all. For many people, needles create a very real psychological barrier. Some people are uncomfortable with them. Some are intimidated by them. Some outright hate them. So even if an injectable version could theoretically improve delivery or absorption, many individuals would still choose the oral option simply because the mental image of self-injection is a complete non-starter. A capsule or tablet simply feels easier, safer, more familiar, and psychologically more manageable for most people. At the same time, oral compounds still have to survive: • stomach acid • digestion • intestinal absorption • and liver processing before the body can actually utilize them systemically. That does not automatically make oral delivery “bad.” But it does raise reasonable questions about how much is truly being absorbed and utilized compared to alternative delivery methods. The problem is we are probably never going to see massive human clinical trials comparing oral versus injectable delivery for most peptides, nutraceuticals, amino acids, or connective tissue support compounds. Not necessarily because the concepts lack scientific merit…but because the economics often do not make sense.
2
0
May 15 •
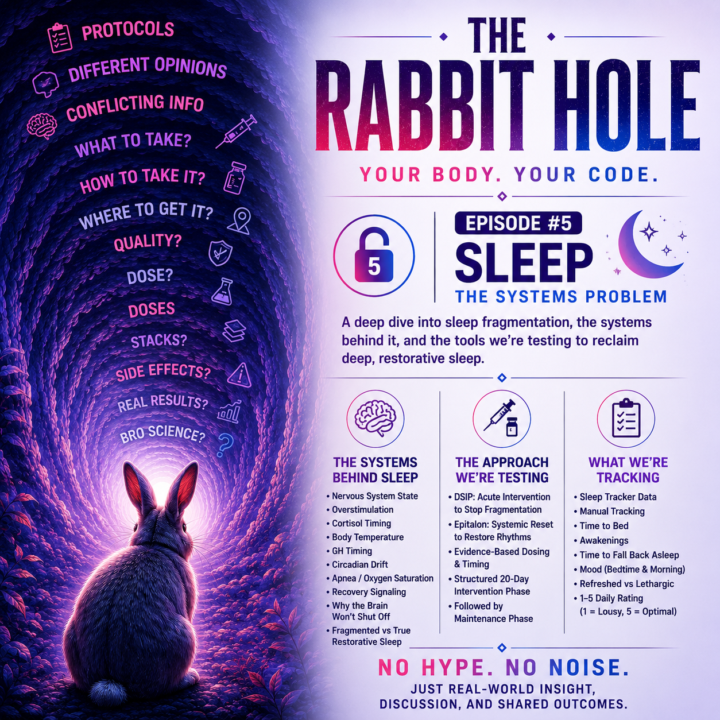
They Call it the Rabbit Hole — "SLEEP" — THE SYSTEMS PROBLEM
Why am I Waking Every 2 to 4 Hours? Why am I exhausted even when I technically slept? Waking up every 2 to 4 hours is a classic symptom of sleep fragmentation, textbook version - It severely truncates your slow-wave (delta) sleep and prevents your brain from clearing metabolic waste. My sleep cycle seems to match this 2-4-hour cycle on any given night. From what I’ve gathered so far, waking every 2–4 hours may reflect a failure to smoothly transition between sleep cycles. Instead of dropping back down into deep slow-wave sleep, a micro-arousal becomes a full awakening My waking up every 2, 3, or 4 hours could mean my brain is failing to seamlessly transition from the end of one sleep cycle back down into the deep, slow-wave sleep of the next cycle. Instead, a micro-arousal triggers a full awakening. At that point I’m usually associating waking with the need to urinate. Half the time it’s not even a real need -- the brain is saying go. So I’ve tried several peptides taken within 30-60 minutes before bed. Some independently or stacked. CJC1295 & Ipamorelin Then the GHRP & GHTh’s potential with Tesamorelin. Tried Neuro next - Selank & DISP. Ran Epitalon a cycle by itself. I had incorporated all the supplements I had researched: Glycine @3-5 grams Magnesium Glycinate @ 250mg nightly. Even brought in L-Theanine @ 200mg when I felt stressed or had traveled. The one trend that I was sure was consistent was my training and diet. That did not really fluctuate. The first few days of a new peptide or stack and yes, I had some benefit, or felt I did. But after a few days to maybe a week, I was right back to the drawing board. I kept thinking sleep was a compound problem, but I’m starting to realize it may actually be a systems problem and so my focus has changed to: nervous system state, overstimulation, cortisol timing, body temperature, GH timing, circadian drift, apnea/oxygen saturation, recovery signaling, why the brain won’t shut off, fragmented sleep vs true restorative sleep.
May 10 •
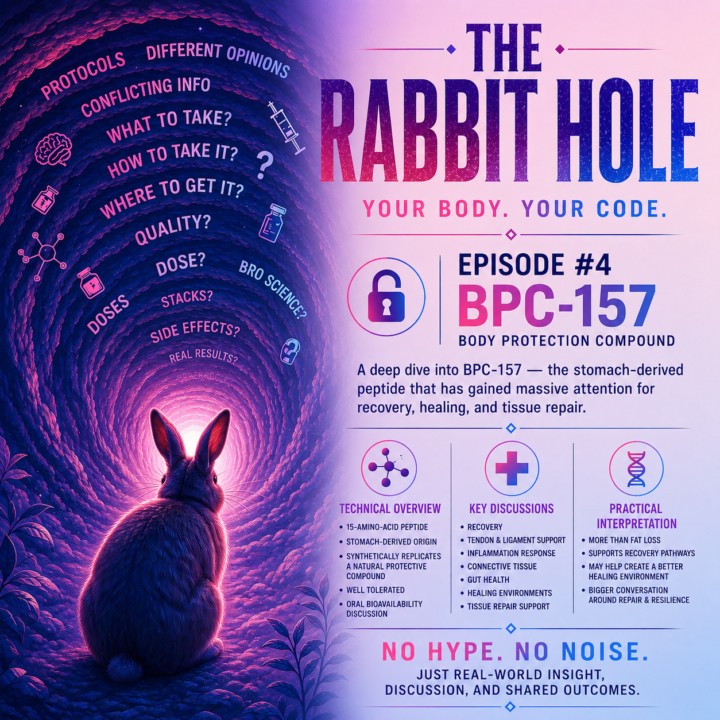
They Call it -- The Rabbit Hole Episode #4
“Wait… Peptides do more than fat loss?” BPC-157 — Technical Overview BPC-157 (Body Protection Compound) is a synthetic 15-amino-acid peptide derived from a protective compound associated with the stomach and gastric system. One thing that made BPC-157 stand out to me early on was learning it originated from our stomachs. In simple terms, it was synthesized to replicate and study a compound already naturally produced by the body. Honestly… BPC-157 was one of the very first peptides that pulled me into this rabbit hole. At the time I wasn’t even looking at peptides for body composition or fat loss. I was researching: • recovery • joint issues • inflammation BPC-157 .“The Body Protection Compound.” That name alone had me think: “Ok… this may actually be something.” Yes… naive at first 😂But the endless amount of content out there corrected that quickly. The more I researched it, the more I kept seeing discussions around: • recovery • tendon & ligament support • inflammation • connective tissue • gut health • healing environments All the conditions and symptoms I had or felt I had. Another interesting part is how far the oral bioavailability discussion has come since I first started researching BPC-157, since most peptide delivery methods were — and still largely are — associated with injections. BPC-157 In simple terms: • 15-amino-acid peptide • stomach-derived origin • recovery discussion • tissue repair support • inflammation response • gut & connective tissue discussion • oral delivery discussion BPC-157 — Practical Interpretation - For me, this was one of the first compounds that made me realize peptides were far more than just "fat loss compounds.” Now the research wasn’t just about my knee and how I could bring relief and balance back to my knee. Suddenly the possibilities started expanding into appetite, food noise, weight loss, body re-composition, sleep and anti-aging. I started seeing what felt like endless possibilities beginning to emerge. And honestly… that’s where the rabbit hole really started for me.
May 7 •
The Rabbit Hole
One thing I’ve realized about getting deeper into peptides… The deeper you go… the less these compounds fit neatly into the labels people give them. A peptide gets labeled:“skin peptide”“fat loss peptide”“healing peptide” But then you start digging into signaling pathways, inflammation, oxidative stress, copper regulation, tissue communication, mitochondrial effects, gene expression… …and suddenly you realize some of these compounds are doing WAY more than the simple label attached to them. GHK-Cu has been one of those for me lately. I originally looked at it through the cosmetic / skin side of things. Now?I’m not even sure “skin peptide” remotely explains what it may actually be involved in. This is the part I geek out over honestly. Getting into the weeds.Looking underneath the marketing labels.Trying to understand the actual signaling environments and why compounds may have broader effects than people realize. Most people probably don’t care to go that deep 😂 But that’s the rabbit hole that keeps pulling me further into this space.
May 7 •
They Call it - " The Rabbit Hole"
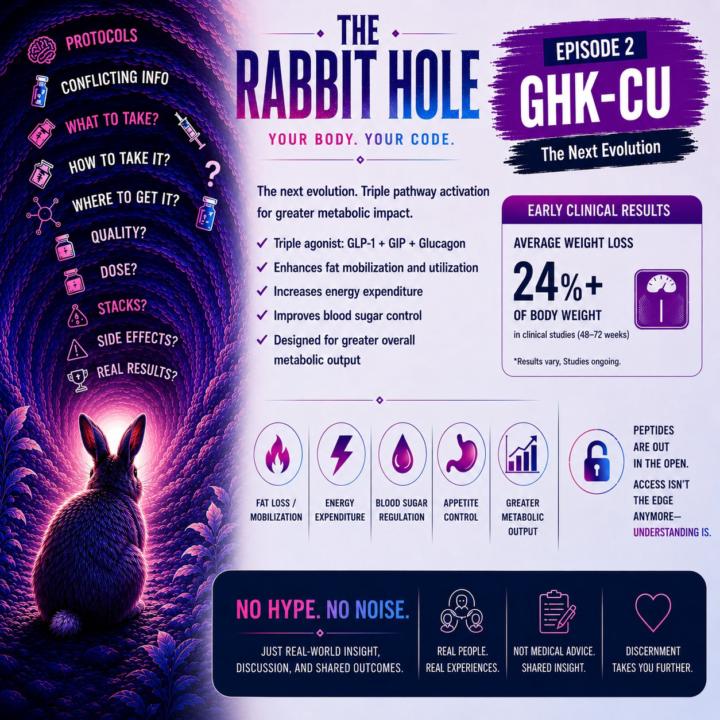
Retatrutide — Technical Overview Retatrutide is an experimental, once-weekly injectable medication currently in Phase 3 clinical trials for weight management and Type 2 diabetes. Often referred to as a “triple agonist,” it targets GLP-1, GIP and glucagon receptors. Unlike Tirzepatide, which is often known for stronger appetite suppression, Retatrutide is gaining attention because of the addition of the glucagon receptor pathway. That third agonist — the glucagon receptor (GCGR) — is what many people consider the potential game changer. The glucagon pathway plays a major role in energy metabolism, particularly around: • fat burning • energy expenditure • metabolic activity • inhibiting fat storage Which is why many people are now referring to Retatrutide as the potential “gold standard” evolution of GLP-based therapies. In simple terms: • Triple agonist • GLP-1 + GIP + Glucagon pathways • Appetite & satiety signaling • Blood sugar regulation • Delayed gastric emptying • Increased metabolic activity Retatrutide — Practical Interpretation • less food noise • less constant hunger • smaller portions • better control around food • easier weight loss For some people it’s the first time in years they feel like they are in control of their body. But eventually another realization starts setting in… Appetite suppression and weight loss are one thing. Rebuilding the foundation underneath is another. Because at some point the real question becomes: What happens when the compound is no longer doing all the heavy lifting? That’s where nutrition, movement, sleep, stress, habits and long-term lifestyle change start becoming the real driver. In many ways, GLP-1s don’t just change body weight. They expose the internal environment and habits that were already there underneath.
1-7 of 7
powered by
skool.com/monument-method-2583
Your Body. Your Code.
The science is out. The code is yours to write.
A place to share real peptide experiences and see what’s actually working.
Suggested communities
Powered by