
Write something

3d •
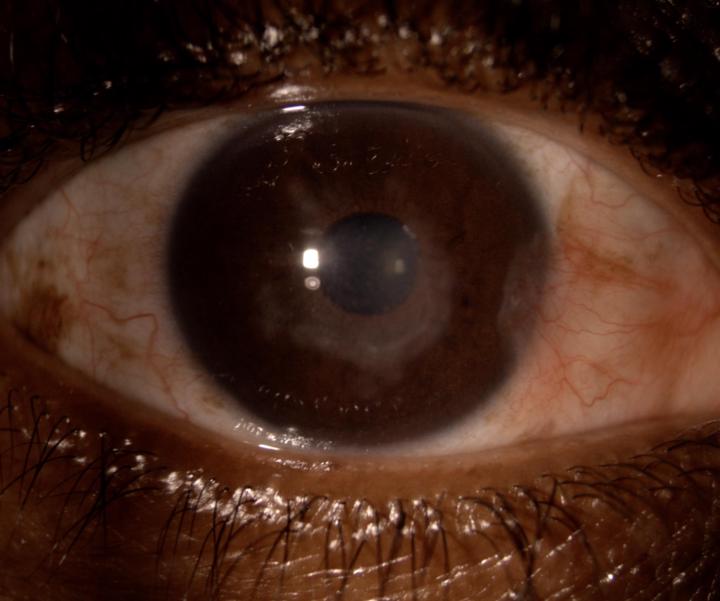
HSV Keratitis: Small Virus, Big Impact on Vision
By Dr Kashmira Rawjee Today’s case is a 41 year old female presenting with reduced visual acuity of 0.5 in the right eye. A diagnosis of immune stromal keratitis was made and the patient was treated with oral acyclovir and topical cortisone. Visual acuity improved to 0.9 in 2 weeks on the above treatment. Disciform keratitis is also known as immune stromal keratitis. The pathophysiology is an immune mediated reaction to Herpes Simplex Virus rather than viral replication and the findings therefore differ from classic dendritic keratitis. Clinically it presents as central stromal oedema with an intact corneal epithelium. There is reduced corneal sensitivity and and only mild discomfort in comparison to disproportionate drop in visual acuity. Keratic precipitates are usually absent and the anterior chamber is quiet. Although the most common presentation is as a disciform keratitis, other forms include linear, diffuse and sectoral. Management consists of systemic antiviral agents in therapeutic doses for 10-14 days and judicious use of topical corticosteroid drops . Intraocular pressure needs to be monitored and close follow up is required to taper the medication depending on the response to treatment. Timely recognition is imperative and prevents mismanagement. Topical steroids can be vision saving but only when paired with appropriate antiviral cover to prevent reactivation.
3
0
Mar 13 •
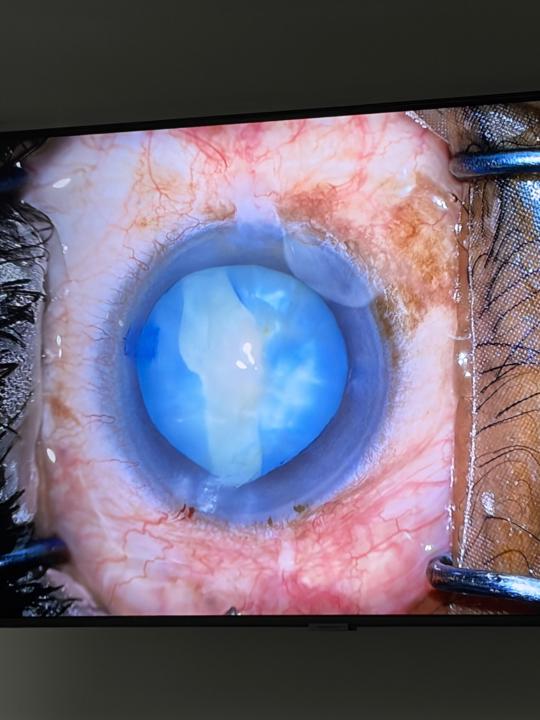
The Argentinian Flag Sign in Cataract Surgery
Mr JM, a 63-year-old patient, presented to our practice with bilateral blindness from dense cataracts. His visual acuity was hand movements in both eyes, leaving him unable to mobilize independently or work to support his family. After waiting two years for surgery at a local hospital, he sought help at our practice—and we were privileged to assist. During surgery we encountered a classic intraoperative sign seen in intumescent white cataracts: the Argentinian Flag Sign. To perform cataract surgery safely, the anterior capsule is often stained with trypan blue to improve visualisation while creating a continuous curvilinear capsulorrhexis—a circular opening in the capsule that allows access to the lens material. In intumescent cataracts, the lens becomes pressurised by liquefied cortex trapped beneath the capsule. When the capsulorrhexis is initiated, the sudden decompression can cause the tear to extend rapidly toward the lens periphery on either side. The resulting pattern—a central white cataract bordered by two blue-stained capsular flaps—resembles the blue-white-blue stripes of the Argentinian flag . Recognizing this sign is critical because uncontrolled capsular extension can lead to: • Extension of the tear to the lens equator or posterior capsule • Risk of lens material dropping into the vitreous cavity requiring retinal surgery • The need to modify surgical technique or convert to a different surgical approach In this case, Dr Kashmira Rawjee used specialised techniques to safely decompress and remove the cataract without vitreous loss or capsular complications. An intraocular lens was successfully implanted in the capsular bag, and the capsulorrhexis was completed. The most rewarding moment came two days after surgery, when Mr JM was able to perform a simple but life-changing task again—walking independently. We look forward to his upcoming postoperative review to see the full visual and functional impact that cataract surgery will have on his life.
Mar 20 •
Small Bump, Simple Fix!
Cyst removal performed by Dr Ashvira Moodley from iSurgeon. Optometrists often spot subtle eyelid lesions during routine eye exams. One that occasionally appears is a hydrocystoma — a benign cyst arising from the sweat glands of the eyelid. In this case: The first image shows a translucent cystic lesion on the lower eyelid. The second image shows the post-removal result, restoring a smooth lid contour. Hydrocystomas are typically fluid-filled, dome-shaped lesions that may appear clear or slightly bluish. They are usually painless but can slowly enlarge and sometimes become cosmetically bothersome for patients. Clinical clues at the slit lamp • Smooth, cystic appearance • Translucent or shiny surface • Often located along the lower eyelid margin or periocular skin • May fluctuate in size with heat or humidity When to refer? If the lesion is growing, atypical, symptomatic, or the diagnosis is uncertain, referral to an ophthalmologist is helpful for confirmation and management. Management: Hydrocystomas are benign and treatment is often straightforward, with simple removal providing both functional and cosmetic improvement. A great reminder of how optometrists and ophthalmologists work together to keep patients seeing — and feeling — their best.
3
0

Jan 14 •
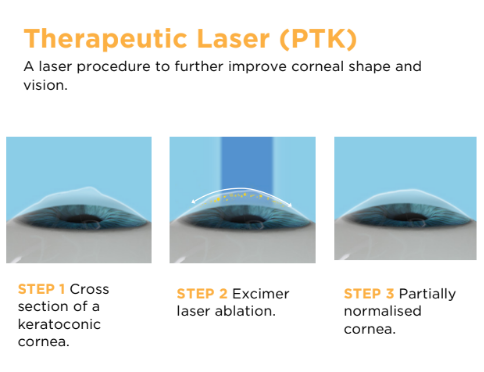
Therapeutic laser in keratoconus to improve quality of vision.
Cross linking often stops progression of keratoconus, however does not improve refractive outcomes. PTK (phototherapeutic keratectomy) uses the same excimer laser used in LASIK and PRK. This laser can be combined with cross-linking in keratoconus patients with a suitable cornea to improve the topography and optics. PTK can be performed at the time of cross-linking to reduce corneal surface irregularities. PTK helps reduce higher-order aberrations and can lead to improved corneal topography and enhanced quality of vision. Suitable patients are those with a pachymetry greater than 450um and lower levels of irregular astigmatism. PTK can also be performed after cross-linking. Below is a case study of patient: History: 21 year old lady with keratoconus progression. We planned to perform a PTK of 50um to reduce the irregularity over the cone. The amount of microns is determined by the epithelial map which allows us to precisely remove a specific depth of epithelium and irregular stroma. Based on this epi map we have decided to go with 50um to remove the epithelium. This was followed by a standard cross-linking. Traditionally in crosslinking we use alcohol to remove the epithelium. Post operative: One can note that the axial map is improved showing reduced K readings. The refraction and visual acuity have also improved: Refraction: Pre Op L) -4.00/-6.00X141 Post Op L) -4.50/-4.75X145 Visual Acuity: Pre Op VAL) 0.6 Post Op VAL) 0.7 Patients undergoing crosslinking combined with PTK will often have good best corrected visual acuity with spectacles and improved quality of vision
Mar 3 •
When the Pupil Won’t Play Along: Tackling Small Pupil Cataracts
This week’s focus: Cataract surgery in patients with small pupils — a scenario that can quickly turn routine into complex. As we know, several patient-specific factors can make cataract surgery more technically demanding: 🔹 Sunken eye / deep orbit 🔹 Small pupil 🔹 Floppy eyelids 🔹 Hard cataract 🔹 Dislocated cataract 🔹 Loose zonules Each of these requires anticipation, planning, and the right tools in theatre. The featured case involves a patient who presented with a grade 3 nuclear sclerotic cataract and reduced visual acuity. - Auto-refraction: -1.00/-0.75X55 - Visual acuity: 0.4 The patient’s pupil failed to dilate despite the administration of intracameral medications, such as Phenylephrine. We subsequently utilized a Malyugin Ring to stretch the pupil. Once the pupil was expanded, we identified pseudoexfoliation as the underlying cause of the miosis. The pupil expander allowed us to perform the surgery uneventfully, avoiding high-risk complications such as iris trauma or dropped nuclear fragments. In addition to managing the small pupil, we accounted for the risk of a myopic surprise with the intraocular lens implant by targeting +0.25 for a distance result. At three days post-surgery, the patient’s uncorrected visual acuity was 0.9 with a refraction of 0.00/-0.50x60 degrees. At iSurgeon, we frequently perform complex cataract surgeries and remain prepared for all potential adverse events. (Video is sped up at 1.5x speed)
2
0

1-9 of 9
