
Write something

29d •
Restoring Vision After Eye Trauma
By Dr Ashvira Moodley A patient recently presented with significantly reduced vision following eye trauma. Examination revealed a subluxed intraocular lens (IOL) — meaning the artificial lens implanted during previous cataract surgery had become displaced from its normal position. At presentation, the patient’s visual acuity was 0.1. Following careful assessment, surgery was performed to remove the unstable lens and implant a posterior iris-fixated Artisan lens (secondary IOL). At the 6-week postoperative visit, the patient’s visual acuity had improved to 0.8, demonstrating a significant restoration of visual function and lens stability. The video below demonstrates the implantation of the secondary intraocular lens (posterior Artisan IOL). What is a subluxed IOL? A subluxed IOL occurs when the lens implant shifts out of position. This can happen due to: - Eye trauma - Weakening of the structures that support the lens - Previous eye surgery - Certain eye conditions affecting the lens support system Symptoms may include: - Blurred or fluctuating vision - Double vision - Glare and halos - Visual distortion Early assessment is important, as timely intervention can help restore vision and prevent further complications.
4
0
Jun 12 •
The Thunderstorm Retina ⛈️
By Dr Kashmira Rawjee This weeks case is a 53 year old female presenting with sudden, painless loss of vision in her left eye. Her visual acuity was reduced to 0.3 in the left eye. On fundus examination, we were greeted by widespread retinal haemorrhages, dilated tortuous veins, cotton wool spots, and optic disc swelling—the classic "blood and thunder" appearance of a Central Retinal Vein Occlusion (CRVO). CRVO typically presents with acute, painless unilateral visual loss, ranging from mild blurring to profound vision impairment. Non-ischaemic CRVO accounts for 75% of cases and results in mild to moderate loss of acuity. Ischaemic CRVO results in profound retinal ischaemia and vision loss to 6/60 or worse. Some patients may also report metamorphopsia or visual field defects. Risk factors include hypertension, diabetes mellitus, hyperlipidaemia, glaucoma, smoking, cardiovascular disease, and hypercoagulable states. In younger patients, an underlying inflammatory or thrombotic disorder should be considered. The consequences can be sight-threatening. Macular oedema is the most common cause of reduced vision, while retinal and iris neovascularisation can lead to neovascular glaucoma and permanent visual loss if not detected and treated promptly. Our patient started a course of Avastin injections for the macular oedema and will continue with treatment until the macula oedema resolves and her vision improves. Further management focuses on identifying and controlling systemic risk factors, monitoring for ischaemia and neovascularisation. Pan-retinal photocoagulation may be required when neovascularisation develops. As optometrists, you are often the first clinicians to identify CRVO. Timely diagnosis, appropriate systemic evaluation, and urgent referral can make a significant difference in visual outcomes.
4
0

May 29 •
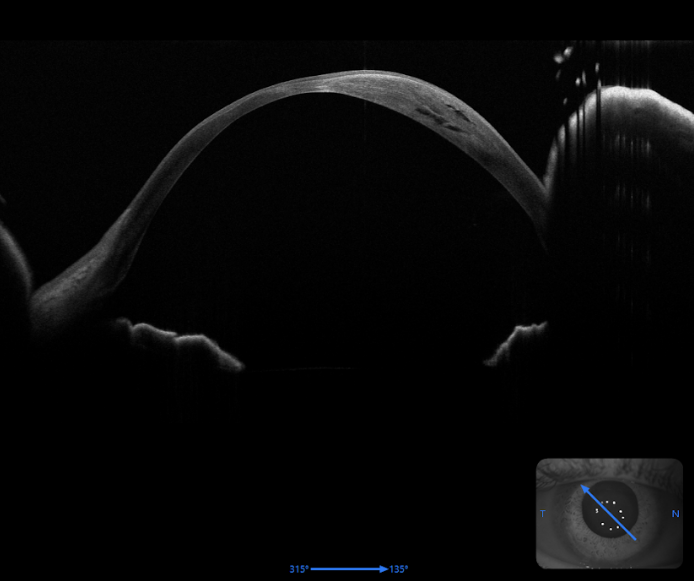
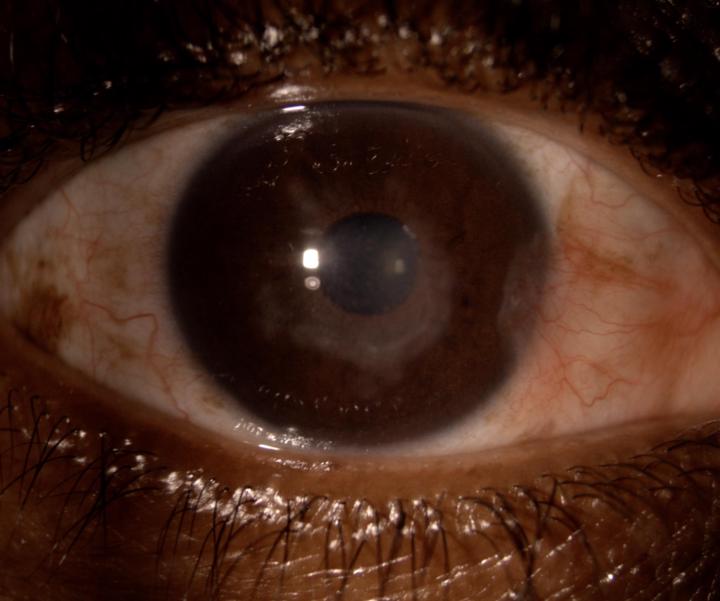
Keratoconus Complication Spotlight: Corneal Hydrops
By Dr Sachin Bawa This week’s case highlights an important complication of keratoconus — corneal hydrops. A young lady (30 years old), known with keratoconus, presented with sudden reduced vision in the right eye. She was initially referred with a possible corneal ulcer. Her background included scleral contact lens wear, with decent visual acuity. Clinical findings showed an oedematous right cornea, with the anterior segment OCT showing oedema in the stroma. A diagnosis of hydrops was made. UVAR) 0.05 ph 0.2 AVAL)0.7 Pachymetry R)244um Her corneas were noted to be very thin, making her unsuitable for corneal cross-linking. She had been managing well with scleral lenses prior to this event. Treatment of the hydrops included the injecting of sulfur hexafluoride (SF6) gas into the anterior chamber. The gas acts as a tamponade, helping to seal the break in Descemet’s membrane. Picture 3 shows her 1 day post op. Historically, hydrops were managed with sodium chloride eyedrops and antibiotic eyedrops. These cases often progressed to corneal scarring, with many patients ultimately requiring a full-thickness corneal transplant. In this case, intervention with SF6 gas injection saved the patient from a corneal transplant. SF6 gas is known to expand and can remain in the eye for approximately 7–14 days, and can assist in expelling the fluid from the cornea and promote healing. A great reminder that timely intervention can completely change the trajectory of these patients Picture 1: Cornea pre-op Picture 2: Cornea post-op picture 3: Slit lamp photo of right eye 1 day post op showing gas bubble.
May 21 •
Small findings. Big clinical significance.
By Dr Ashvira Moodley. Today’s patient presented with a sectoral red eye associated with mild discomfort and irritation, but notably without significant discharge, photophobia, or visual disturbance. On slit lamp examination, the inflamed vessels blanched with topical phenylephrine — a positive phenyl test — supporting a diagnosis of episcleritis rather than scleritis. Episcleritis is a relatively common, benign, and often self-limiting inflammation of the episcleral tissue. Patients typically present with: • Sectoral or diffuse redness • Mild tenderness or irritation • Little to no pain • Normal visual acuity One of the most useful clinical pearls in differentiating episcleritis from scleritis is the phenylephrine blanching test: - Superficial episcleral vessels blanch with phenylephrine - Deeper scleral vessels remain injected in scleritis This distinction is important because while episcleritis is usually benign and manageable with supportive treatment or topical anti-inflammatory therapy, scleritis can be vision-threatening and may be associated with underlying systemic autoimmune disease. A good reminder that careful examination of the “simple red eye” can make all the difference.
4
0

Apr 24 •
HSV Keratitis: Small Virus, Big Impact
By Dr Kashmira Rawjee Today’s case is a 41 year old female presenting with reduced visual acuity of 0.5 in the right eye. A diagnosis of immune stromal keratitis was made and the patient was treated with oral acyclovir and topical cortisone. Visual acuity improved to 0.9 in 2 weeks on the above treatment. Disciform keratitis is also known as immune stromal keratitis. The pathophysiology is an immune mediated reaction to Herpes Simplex Virus rather than viral replication and the findings therefore differ from classic dendritic keratitis. Clinically it presents as central stromal oedema with an intact corneal epithelium. There is reduced corneal sensitivity and only mild discomfort in comparison to disproportionate drop in visual acuity. Keratic precipitates are usually absent and the anterior chamber is quiet. Although the most common presentation is as a disciform keratitis, other forms include linear, diffuse and sectoral. Management consists of systemic antiviral agents in therapeutic doses for 10-14 days and judicious use of topical corticosteroid drops . Intraocular pressure needs to be monitored and close follow up is required to taper the medication depending on the response to treatment. Timely recognition is imperative and prevents mismanagement. Topical steroids can be vision saving but only when paired with appropriate antiviral cover to prevent reactivation.
5
0
1-13 of 13
