
Write something

22h •
📦 Bulk Wholesale Peptides from Orion Peptides – A Quick Guide
Yes, Orion Peptides offers bulk wholesale purchasing for researchers needing larger volumes of research-grade peptides. What Bulk Typically Means: - Larger vial quantities (10–100+ vials) - Higher milligram amounts (50mg, 100mg+) - Custom synthesis projects How to Inquire: 📧 Email:[email protected] 🌐 Website:OrionPeptide.com Provide: 1. Specific peptide(s) 2. Quantity needed 3. Timeline & purity requirements Key Considerations: - Batch-specific COAs available for verification - Strictly for laboratory research & in-vitro testing - Ensure compliance with institutional guidelines 🔬 For research-grade peptides in bulk, check OrionPeptide.com. ⚠️ Research only. Not for human consumption.
0
0


1d •
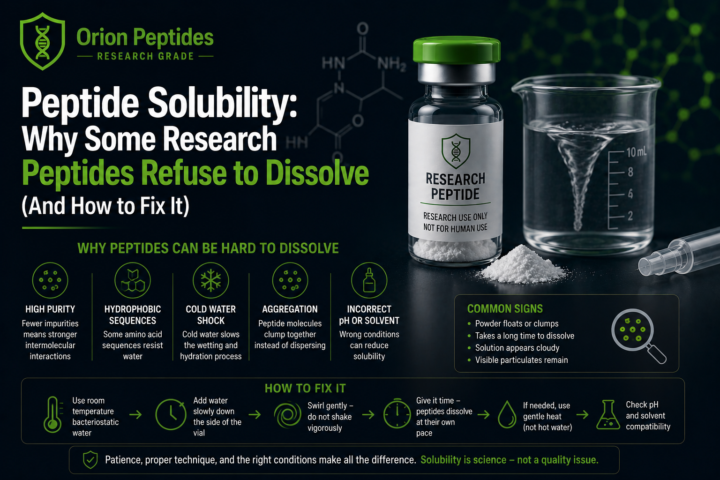
Peptide Solubility: Why Some Research Peptides Refuse to Dissolve (And How to Fix It)
One of the most common questions in peptide research isn't about dosing or storage—it's about reconstitution. A researcher adds bacteriostatic water to a vial, waits a few minutes, gives it a gentle swirl... and nothing happens. The peptide remains cloudy, forms small particles, or appears to stick stubbornly to the bottom of the vial. The first assumption is usually that something is wrong with the peptide. In reality, that's often not the case. Peptide solubility is influenced by chemistry, molecular structure, purity, salt form, and even the way the peptide was freeze-dried. Some compounds dissolve almost instantly, while others require considerably more patience and a slightly different approach. Understanding why this happens can prevent unnecessary frustration and help preserve valuable research materials. Why Some Peptides Dissolve Instantly While Others Don't Every peptide has its own unique chemical personality. Some are naturally hydrophilic (water-loving), while others contain long stretches of hydrophobic (water-repelling) amino acids. When water is introduced, hydrophilic peptides readily interact with the solvent. Hydrophobic peptides, however, prefer interacting with each other instead of the surrounding water molecules. This causes aggregation, cloudiness, or slow dissolution. The longer and more complex the peptide becomes, the greater the likelihood of this occurring. This is why compounds like: - Tesamorelin - Kisspeptin-10 - IGF-1 LR3 - Certain lipidated GLP-1 analogues often require additional care during reconstitution compared to smaller peptides like BPC-157 or TB-500. Tesamorelin: Why It Can Take Time Tesamorelin contains 44 amino acids. For comparison, many popular research peptides contain fewer than 15. That additional length creates several challenges. Longer peptide chains can begin folding into secondary structures such as alpha helices, exposing hydrophobic regions that naturally stick together. Tesamorelin also contains an N-terminal lipid modification which further reduces water solubility.
1d •
Why Higher Purity Peptides Can Be Harder to Dissolve: The Science Behind Reconstitution
Most researchers assume that higher purity automatically means easier handling. Surprisingly, that's often not the case. If you've ever opened a vial of a 99%+ HPLC peptide, added bacteriostatic water, and watched it remain cloudy, form a gel, or leave stubborn particles at the bottom of the vial, you may have wondered whether something was wrong with the product. In many cases, nothing is wrong at all. In fact, the highest-purity peptides are often the most challenging to dissolve. Rather than indicating poor quality, difficult reconstitution is frequently the result of advanced purification techniques and the underlying chemistry of peptides themselves. Understanding why this happens can save researchers frustration and help ensure consistent preparation of research materials. Purity Doesn't Always Mean Easy Reconstitution Peptides are manufactured through solid-phase peptide synthesis (SPPS) before undergoing purification, typically using high-performance liquid chromatography (HPLC). The goal of purification is simple: Remove everything except the desired peptide. That includes: - Truncated peptide fragments - Incomplete sequences - Residual protecting groups - Reaction by-products - Residual synthesis chemicals - Various peptide impurities When purification reaches 99% or greater, almost every impurity has been removed. Ironically, many of those impurities actually helped keep the peptide easier to dissolve. Why Impurities Can Improve Solubility This sounds backwards, but impurities often prevent peptide molecules from sticking tightly together. Lower-purity batches contain small peptide fragments that naturally separate the larger molecules inside the lyophilized cake. Think of them as tiny spacers. When these spacers disappear during purification, identical peptide molecules pack together much more efficiently. The result is stronger intermolecular interactions, including: - Hydrophobic interactions - Hydrogen bonding - Molecular stacking - Aggregate formation
1
0

1d •
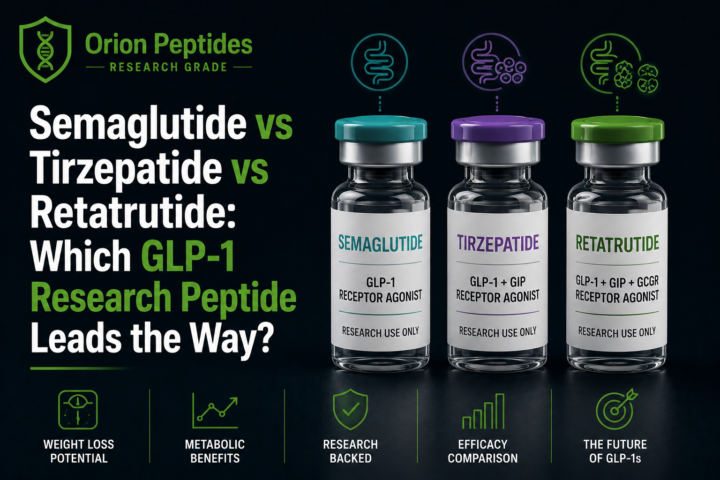
Semaglutide vs Tirzepatide vs Retatrutide: Which GLP-1 Research Peptide Leads the Way?
GLP-1 receptor agonists have transformed metabolic research over the past decade. What began with single-receptor compounds has rapidly evolved into dual and now triple agonists capable of targeting multiple metabolic pathways simultaneously. Today, semaglutide, tirzepatide, and retatrutide represent the three major generations of incretin-based research peptides. While all three influence appetite regulation and glucose metabolism, they differ significantly in receptor activity, research maturity, and the metabolic effects observed in published studies. In this guide, we'll compare the latest evidence surrounding each compound, explain how they work, examine their strengths and limitations, and discuss where metabolic research appears to be heading. The Evolution of GLP-1 Research The progression has been remarkably rapid. Researchers first demonstrated that activating the GLP-1 receptor alone could dramatically improve glucose regulation and reduce body weight. The next generation expanded beyond GLP-1 by activating the GIP receptor, producing even greater metabolic effects. The newest generation adds glucagon receptor activation, creating an entirely new approach to energy expenditure and metabolic flexibility. Each generation attempts to solve one question: Can activating additional metabolic pathways produce better outcomes than GLP-1 alone? Current research suggests the answer may be yes. Semaglutide: The Foundation of Modern GLP-1 Research Semaglutide, developed by Novo Nordisk, remains the most extensively studied GLP-1 receptor agonist available. Its molecular modifications allow a half-life of approximately one week, making once-weekly administration possible in research settings. Mechanism of Action Semaglutide selectively activates the GLP-1 receptor, leading to several well-characterized downstream effects: - Glucose-dependent insulin secretion - Reduced glucagon secretion - Delayed gastric emptying - Central appetite suppression - Reduced food intake - Improved glycemic regulation
0
0
1d •
Purity Alone Does Not Equal Safety: The Peptide Tests That Actually Matter
When researchers evaluate a peptide product, purity is usually the first number they look at. 99% purity. 98% purity. 99.5% purity. The higher the number, the better the product must be, right? Not necessarily. One of the biggest misconceptions in the peptide industry is that purity alone determines quality. In reality, a peptide can have impressive purity results while still failing some of the most important safety and quality tests available. If given the choice between a peptide that is 99% pure but fails sterility testing and a peptide that is 90% pure but passes sterility and endotoxin testing, many experienced researchers would choose the latter every single time. Here's why. What Does Peptide Purity Actually Measure? Purity testing, usually performed using High-Performance Liquid Chromatography (HPLC), measures how much of the sample consists of the intended peptide compared to other compounds. For example: - 99% purity means approximately 99% of the measured material matches the target peptide profile. - 95% purity means roughly 95% matches the target peptide profile. - 90% purity means approximately 90% matches the target peptide profile. This information is valuable. Researchers want to know that they are receiving the compound they ordered. However, purity testing only tells part of the story. A purity report does not automatically tell you: - Whether bacteria are present. - Whether endotoxins are present. - Whether the product was manufactured in a sterile environment. - Whether contamination occurred during filling. - Whether the product was stored properly. - Whether the product contains pyrogens that could trigger inflammatory reactions. Purity answers one question: "Is this the correct molecule?" It does not answer: "Is this product safe and clean?" The Hidden Problem With Chasing Purity Numbers Many researchers become obsessed with purity percentages. A product advertised as: - 99.8% purity often sounds dramatically better than one advertised as:
0
0

1-30 of 1,085
powered by

skool.com/biohacking-and-longevity-group-3757
All-in-one peptide education community. 🧪
Dosing guides, storage protocols, stacking frameworks, vendor intel, GLP-1 research, and expert support.🧬
Suggested communities
Powered by