Activity
Mon
Wed
Fri
Sun
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
What is this?
Less
More
Owned by Travis
For adults 35+ ready to build muscle, burn fat, and optimize hormones. Aging is inevitable. Decline isn’t. Train smarter. Optimize everything.
Memberships
Fowl
5k members • Free
Built With // MS
21 members • Free
AI Money Lab
88.2k members • Free
The Iron Forge Brotherhood
45k members • Free
Dirt To Dollars
2.6k members • Free
Wholesaling Real Estate
79.9k members • Free
Research Radar
11.8k members • $10/month
Skoolers
161.4k members • Free
Project Biohacked - Peptides
14.1k members • Free
231 contributions to BioOptimization Collective

4h •
What Is "Food Noise?"
One phrase you'll hear over and over is... "Retatrutide got rid of my food noise." But what does that actually mean? Food noise isn't a medical diagnosis. It's a term many people use to describe constant thoughts about food. For some people, it sounds like: • "What's my next meal?" • "I just ate... why am I still hungry?" • "I can't stop thinking about snacks." • "I know I'm full, but I still want to eat." Many people describe food noise as mentally exhausting. That's one reason researchers are interested in therapies that affect appetite regulation. 👇 Question: Before today, had you ever heard the term "food noise?" Yes or No? @Shelby Hollister @Breeann Tegen @Bill Haynes
0
0
1d •
What Are People Actually Saying?
I've spent a lot of time reading through Reddit discussions, and a few themes keep coming up. People commonly say they're interested in Retatrutide because they're hoping for: • Less food noise • Better appetite control • Fat loss • Better body composition Others say they're simply curious because it's one of the newest peptides being studied. Remember... Those are personal experiences and opinions, not scientific proof. That's why it's important to separate what people are reporting from what research has actually demonstrated. 👇 What's the biggest claim you've heard about Retatrutide?
0 likes • 1d
Here are the top 3 claims on Reddit. - Retatrutide burns fat through more than appetite suppression. - It may produce the best overall body recomposition of any current GLP-1–based therapy. - Muscle preservation is possible, but it's driven more by training and nutrition than by the drug itself.
2d •
The Most Confusing Thing About Peptides Isn't the Peptide... It's the Label.
Let's clear up one of the biggest beginner questions. When people see a vial, they usually see numbers like: - 5 mg - 10 mg - 15 mg Then they hear people talking about: - mL - IU - Units It's easy to think they're all the same thing. They're not. Here's the simple version: mg = How much peptide is in the vial. mL = How much liquid is added. IU (or units on an insulin syringe) = A way to measure the liquid after it's been mixed. Those three numbers mean completely different things. Once you understand that, peptide math becomes much less intimidating. Which one has confused you the most?
Poll
3 members have voted
0
0
Mar 23 •
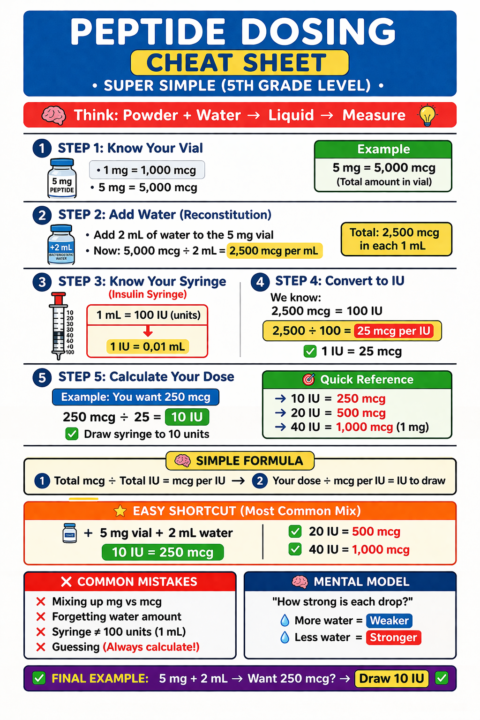
Nobody Understands Peptide Dosing Until This Simple Trick
Peptides start as a powder that must be mixed with water so you can measure them in a syringe. Once mixed, you divide the total amount into the syringe units to know how many micrograms are in each unit, which tells you exactly how much to draw for your dose. Bio-Opt Tracking/Reconstitution Calculator: https://peak-bio-path.base44.app
0 likes • Jun 15
@Melisa Hubbard you're welcome!
0 likes • 5d
@Don Whisenant thank you! 😊
5d •
How Can Something So Small Have Such a Big Impact?
One of the biggest misconceptions about peptides is that they're magic. They're not. Think of a peptide like a key. Your body has millions of locks, called receptors. When the right peptide connects with the right receptor, it sends a signal. That signal may tell your body to do something specific, depending on the peptide being studied. Different peptides send different messages. Some are being researched for metabolism. Some for recovery. Some for growth hormone release. Some for skin health. The important thing to understand is this... Peptides don't force your body to do something. They work by interacting with natural biological pathways that researchers are studying. That's why not every peptide is designed for the same goal. 👇 Question: Before today, did you know peptides worked by sending signals in the body?
1-10 of 231

@travis-dickey-2146
I’m here for people 35+ who refuse to decline. We’ll optimize body, mind & business to reclaim power & build a legacy.
Active 4h ago
Joined Aug 24, 2025
Powered by