Activity
Mon
Wed
Fri
Sun
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
What is this?
Less
More
Memberships
ST3
1.5k members • Free
11 contributions to ST3

May 11 •
NEW COURSE ALERT! High-Functioning Alcoholism and Recovery Illusions
🚨 NEW COURSE RELEASE 🚨 High-Functioning Alcoholism and Recovery Illusions is now available. This powerful 2 hour course explores the hidden side of alcohol addiction where external success, professional achievement, financial stability, or “having it together” can mask the severity of the problem underneath. Many individuals struggling with alcohol use continue to maintain careers, relationships, responsibilities, and daily functioning, creating the illusion that things are under control. This course examines the dangerous patterns of denial, minimization, rationalization, and perceived control that often keep people stuck and untreated for years. Participants will explore:• High-functioning alcoholism and hidden addiction patterns• Recovery illusions and false stability• Denial, minimization, and distorted self perception• Counselling considerations for accurate assessment• Engagement strategies for resistant or high-performing clients• Clinical insight development and treatment planning This training is ideal for addiction professionals, counsellors, peer workers, mental health staff, students, and anyone wanting a deeper understanding of how addiction can hide behind achievement and appearance. ✅ 2 Hour Course ✅ Only $25 USD ✅ Fully Online and Self-Paced ✅ Buy it right here on Skool for $25 USD and it will be instantly loaded to your classroom Sometimes the most dangerous addictions are the ones nobody recognizes because everything still “looks fine” on the outside. See you in the course!


0 likes • May 12
Great subject to address! Will be taking this one as well.
May 8 •
NEW COURSE! AI Companions and Virtual Relationship Dependency
🚨 NEW COURSE RELEASE 🚨 AI Companions and Virtual Relationship Dependency is now available directly in your classroom! This new 3 hour training explores the rapidly growing reality of emotional and relational dependency on artificial intelligence companions, chatbot attachment, and virtual relationships in today’s digital world. As AI becomes more integrated into daily life, addiction and mental health professionals are beginning to encounter clients forming deep emotional bonds with virtual systems. This course examines the psychological drivers behind these attachments, the ethical concerns surrounding AI companionship, and the clinical implications for assessment, treatment, and behavioral addiction support. Topics include: • Emotional dependency and attachment to AI• Behavioral addiction patterns in virtual relationships• Loneliness, trauma, and unmet emotional needs in digital attachment• Ethical and clinical considerations for professionals• Assessment and treatment implications in evolving digital environments• The future of AI relationships and mental health care ✅ 3 Hour Course ✅ $39 USD ✅ Eligible for CE hours ✅ Fully Online and Self Paced ✅ Instant Access Upon Registration Once payment is completed, the course is immediately added to your Skool classroom so you can begin right away. To register, scroll to your classroom to access the course today. This is a really mind altering course, I can't wait to see you there! Dr. C
0 likes • May 8
Love it! Will definitely be taking this course after my weekend rotation.
May 2 •
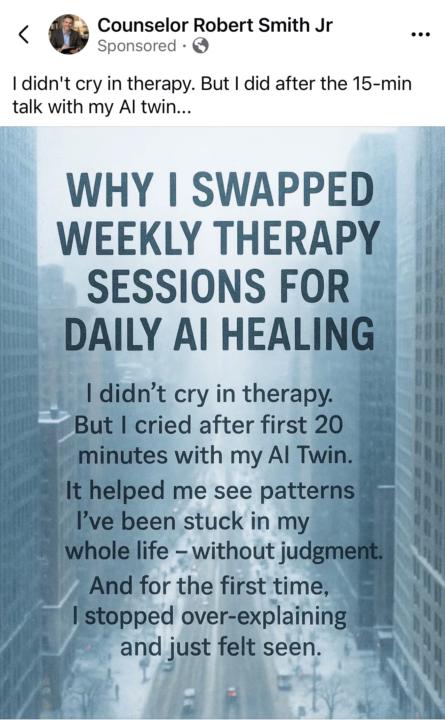
I think I’m still flabbergasted after reading this
I was just scrolling social media because there’s a huge storm outside and I’m trying to have a restful afternoon when I came across the post below. I gasped, loudly. So much so that my dog came in to check if I was OK.. What’s your first reaction when you see this?
1 like • May 5
@Tammy Purdy managed care on steroids. “Can we free up any beds today?”, “Doesn’t that client already have a plan? It’s time to DC”, “How many referrals have been made?” I wish we could slow down and take a beat. Great post, Tammy!
1 like • May 5
@Rhonda Thiemann I do try to accept everyone’s posts, and I’ve been struggling with this, so I’m just going to respond by saying I’ve met, and worked with folks who live with prosthetic limbs. I’ve literally seen them reclaim their agency, and happiness by having a prosthetic. A perfect example of how technology improves people’s lives. Maybe I’m confused at what I read to be a pejorative comment. If I misunderstood, I apologize. Could you elaborate?

0 likes • May 2
Welcome, William!
Apr 22 •
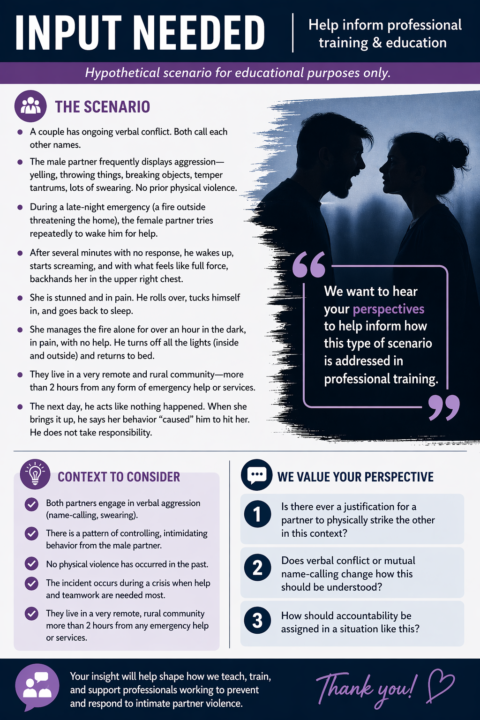
HELP INFORM OUR NEXT FREE INTIMATE PARTNER VIOLENCE COURSE CONTENT!
We are working on informing our next Intimate Partner Violence Training. Can you help us with your input? All replies will be considered. We value all input and hope to receive a variety of answers to help form our training! PLEASE CLICK THE GRAPHIC BELOW SO THAT YOU CAN READ IT IN ITS ENTIRETY. You can comment here, send me a personal DM, or send us an email with your reply to this scenario. We are really trying to work through whether there is ANY Justification of ANY kind to the assault in this scenario that can be warranted. ( Ya'll keep asking us for these scenarios in training so we are looking to you to help us TRY to find these scenarios. I want you to try really hard to warrant this one, but we still want to hear from you if you try and you can't!) You can reach us directly at [email protected] Thank you!
0 likes • Apr 22
There is absolutely no justification in this man hitting his wife. There is no justification in any person hitting their partner. Of course, there’s the discussion of defending oneself, but that is another conversation with a plethora of nuances. Which, of course, is beyond the scope of this poster.
1-10 of 11
@steven-tweedale-4213
Addiction Counsellor at St. Joe’s hospital in Hamilton, ON
Active 14d ago
Joined Mar 25, 2026
Powered by