Activity
Mon
Wed
Fri
Sun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
What is this?
Less
More
Owned by Erik
Direct primary care gives unlimited access to your doctor, same-day visits, clear pricing, and no insurance—medicine built on trust.
Memberships
Skoolers
170.3k members • Free
18 contributions to FirstCall DPC

Apr 13 •
What Does a Real Optimization Program Look Like Inside a DPC Practice?
Most Direct Primary Care practices start with the same mission: Restore time.Restore access.Restore the doctor–patient relationship. But once that relationship is strong, the conversation changes. Patients stop asking only:“Can you treat this problem?” They begin asking:“How do I prevent the next problem?”“How do I improve energy, recovery, and metabolic health?”“How do I maintain muscle as I age?”“How do I reduce cardiovascular risk before disease develops?”“How do I optimize hormones responsibly?”“How do I objectively measure progress?” This is where structured optimization belongs inside the DPC model. Not guesswork.Not supplement stacks based on social media trends.Not protocol mills. Structured. Strategic. Physician-Led. Core Philosophy of FirstCall Optimization™ Optimization is not motivation.Optimization is measurement, interpretation, and adjustment. We focus on identifying physiologic constraints and systematically improving them over time using objective data. Key principles: • longitudinal biomarker tracking • individualized treatment decisions based on clinical context • structured reassessment intervals • avoidance of unnecessary polypharmacy • integration of lifestyle, nutrition, sleep, and training variables • ethical hormone optimization when appropriate • transparency with patients regarding expected magnitude of benefit Optimization should improve healthspan markers without compromising long-term safety. Core Components of the Program 1. Structured Lab Cadence We track biomarkers at defined intervals rather than ordering random labs reactively. Typical cadence: Baseline16 weeks32 weeksAnnual reassessment Focus areas often include:metabolic markerslipids and cardiovascular risk markershormonal balancethyroid physiologymicronutrient statusinflammation markersinsulin sensitivity markers The objective is trend analysis, not isolated lab interpretation. 2. Genetic Insight (3X4 Genetics) Genetics informs risk architecture but does not dictate destiny.
Poll
Cast your vote
0
0
Apr 12 •
Community-Based Performance Medicine: A Strategic Outreach Model for DPC Practices
Most Direct Primary Care practices talk about prevention. Few operationalize it in a way that measurably improves outcomes while strengthening community trust. One highly effective strategy: Performance Medicine programs for high school athletes. This is not about supplements or selling services. This is about guiding developing athletes toward evidence-based optimization while protecting them from the rapidly growing black-market peptide ecosystem. The Problem Most Communities Don’t Realize Exists High school athletes are increasingly exposed to: - Social media-driven “optimization” messaging - Peer discussions about SARMs, peptides, and research chemicals - Influencers promoting unregulated compounds - Online vendors selling products labeled “not for human consumption” - Misunderstanding of legal vs illegal performance enhancement Many families assume their athletes are only using protein powder and creatine. That assumption is frequently incorrect. Without physician-led education, athletes often obtain: - Unverified peptides - Underground SARMs - Hormonal compounds - Contaminated supplements - Improper dosing protocols These introduce real risks: - Endocrine suppression - Fertility impact - Liver toxicity - Psychiatric effects - Impaired long-term athletic development Where DPC Has a Unique Strategic Advantage Direct Primary Care physicians have the flexibility to engage proactively in their communities without insurance constraints dictating care delivery models. Performance Medicine outreach allows practices to: - Establish early relationships with families - Provide objective, science-based guidance - Position the physician as the trusted authority - Create long-term continuity of care - Improve public health literacy This is preventive medicine in its purest form. What a Community-Based Athlete Optimization Initiative Can Include 1. Education First, Not Intervention First Host informational sessions for:
0
0


Mar 4 •
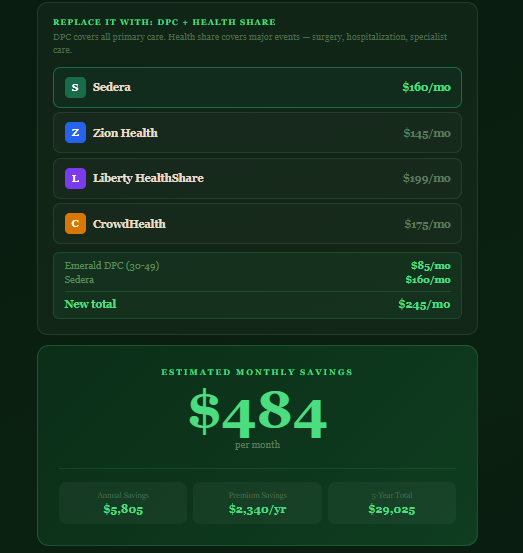
Show patients the value of DPC
I built this app in 20 minutes--it's amazing what we can do now! The point of this is to show potential patients the amount of money that they could save with DPC combined with Health Share compared to insurance. Some people need to see it to believe it. https://24-7-bot.harmonyopsfordpc.com/savings
0 likes • Mar 4
Great post Anne!!
Mar 1 •
What Niches Actually Work Well Inside Direct Primary Care — And Why
What Niches Actually Work Well Inside Direct Primary Care — And Why One of the most common questions I get is: “What niches work best in DPC?” Men’s health. ADHD. Weight loss. Peptides. Hormone optimization. Longevity panels. The question isn’t whether these niches “sell.” The better question is: Do these niches align with the structural strengths of the DPC model? Because DPC is not just a pricing model. It’s an infrastructure model. Certain niches work exceptionally well inside DPC not because they are trendy — but because they require exactly what DPC is designed to deliver: - longitudinal oversight - rapid access - relationship continuity - flexible communication - high-trust decision making Let’s break down why some of these niches fit naturally inside DPC. 1. Men’s Health / Testosterone Optimization This works well inside DPC for one simple reason: It is longitudinal and requires nuance. Testosterone management is not a one-visit prescription event. It requires: - lab monitoring - dose adjustment - symptom interpretation - lifestyle integration - risk stratification In traditional insurance-based primary care, there is rarely time to do this well. Visits are short. Follow-up is fragmented. Messaging is inefficient. DPC solves that. When structured correctly, men’s health becomes: - predictable follow-up - scheduled labs - protocol-based monitoring - defined communication boundaries It fits the model — as long as capacity is engineered. 2. ADHD Management ADHD is another niche that aligns with DPC’s strengths. Why? Because ADHD care requires: - frequent check-ins - medication titration - behavioral discussion - rapid response for side effects - documentation consistency In traditional systems, these patients get lost in the shuffle. Refill friction creates frustration. Follow-up is delayed. In DPC, with structured refill cycles and defined boundaries, ADHD management becomes stable and predictable.
Mar 1 •
🔥 Capacity Is the Product
🔥 Capacity Is the Product Direct Primary Care is often described as an access model. It isn’t. It is a capacity model. And the sooner that distinction is understood, the sooner a DPC practice becomes stable, sustainable, and intellectually honest. In traditional insurance-based primary care, physician capacity is fragmented and obscured. The system absorbs inefficiency through layers of bureaucracy, referrals, billing friction, institutional policy, and administrative overhead. There is waste everywhere, but there is also buffering. DPC removes the waste. But it also removes the buffer. What remains is pure capacity. Your time. Your cognitive bandwidth. Your emotional energy. Your boundaries. When a physician launches a DPC clinic, they often ask: How many members can I support? The better question is: How much capacity do I actually have? These are not the same. Capacity is not simply the number of visits you can schedule in a week. Capacity is multi-dimensional and dynamic. It includes: Time Capacity The number of meaningful clinical interactions you can sustain without compressing visits or eroding depth. Cognitive Capacity The number of longitudinal patients you can track without mental spillover — the quiet accumulation of unfinished threads that follow you home. Emotional Capacity The amount of direct-access medicine you can provide before enthusiasm turns into obligation. Boundary Capacity The volume of texts, calls, and asynchronous clinical decisions you can absorb before they begin to create invisible workload. In a DPC model, these dimensions compound. Because in DPC, there is no dilution. There is no RVU-driven fragmentation. There is no system absorbing the overflow. There is no institutional latency to hide inefficiencies. The physician becomes the central processing unit of the system. If that processing unit is not engineered with intention, failure modes are not random. They are predictable. They look like: - Response-time anxiety - Gradual visit compression - The slow expansion of “quick questions” - Text fatigue that is difficult to name - Subtle resentment toward the very access you promised - Burnout inside a model that was supposed to prevent burnout
1-10 of 18

@erik-petersen-8842
FirstCall DPC: real doctors, direct access, same-day care. No insurance games—just transparent, personal medicine that puts patients first.
Active 58d ago
Joined Dec 21, 2025
Santa Rosa Beach, FL
Powered by