Activity
Mon
Wed
Fri
Sun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
What is this?
Less
More
Owned by Anne
Memberships
SaaS University (GoHighlevel)
7.3k members • Free
Automated Marketer
4.3k members • Free
STR/MTR Investing for Doctors
560 members • Free
Bossdoctors
50 members • Free
FirstCall DPC
78 members • Free
AI Builders Circle
529 members • Free
Disrupter Academy
4.2k members • $9/month
The Owner's AI Room
718 members • Free
HighLevel Quest
14.4k members • Free
9 contributions to FirstCall DPC

May 10 •
AI and Social Media Content Creation
I fully support using AI to assist in creating content, but only in the right way. I can tell in seconds who used chatGPT to write their content and didn’t bother to edit or try to make it sound like them. That’s not the right way. To create engaging content that sounds like YOU, it’s important to teach AI what you sound like. Start by uploading some of your writing into your favorite LLM, my favorite is Claude right now. Even better, chat with Claude and ask it to interview you to create your “brand voice.” You can identify your ideal patient, what you do for them, why they should come to see you, what are the benefits. You want to lead with what are your ideal patient’s pain points, and how do you help alleviate those pain points. Don’t focus on the features of your practice, focus on the outcomes. Then when AI helps create captions for you, it knows what you do and what you stand for. After the first iteration of content, review and edit. Change around words every sentence or two. Remove the long dashes and sub a comma or period, whatever makes sense. Remove the repetitive short statements if you don’t talk like that. Look out for the constant lists of 3 things and adjust if needed. Those are a few of the telltale signs of AI generation. You don’t have to change everything, but you don’t want to post the first thing it spits out. It’s not so scary to post on social media. You just have to jump in knowing your first posts will be bad. And that’s ok! You will get better the more you create and post. If you use automations, then you can create and schedule a month’s worth of posts and you don’t need to touch it again for a month. So if posting on social media about yourself or your practice makes you want to run away, that’s normal. Take a look at the Social Media Sprint that I made for DPC docs. It walks you through creating your brand voice and uses automations to post for you on a schedule. Here’s a link to learn more 😊 https://reach.harmonyopshealth.com/sprint-home
2
0
Apr 11 •
Social Media Sprint!
I hear from so many DPC docs that they hate social media. After a day full of caring for your family, patients, running your DPC, now it's 11pm and you're trying to figure out what to post on Instagram because you didn't get to it earlier. And honestly, sometimes you avoid posting because it's just not your thing, but you know it helps. That's exactly why the Social Media Sprint exists. It's a 14-day social media jumpstart beginning April 20th. Harmony Ops handles it all in one place: using a list of guided prompts, AI writes captions that sound like you, you approve them, and you post on up to 7 different social media platforms from one central page. Takes about 2-3 hours of setup and you'll have two weeks of posts scheduled & ready to go. You don't have to touch it after that. Plus your own branded "Is DPC Right for Me?" calculator page that educates prospective patients, crunches the numbers for them, and drives them straight to your door.When the sprint ends you keep the brand voice guide, posting planner, content guide, and all the posts to reuse anytime. $99. Cart closes April 18th. The only thing easier than this is paying someone else to do it entirely. And that costs a lot more than $99. https://reach.harmonyopshealth.com/sprint-home-page
1
0

Mar 15 •
Independent Practice Path - starts March 24
Many docs who are interested in Direct Primary Care spend a long time in the research phase. I call it "Procrasti-learning." Endlesslessly reading, listening to podcasts, joining groups, trying to figure out where to start, or waiting until everything is "perfect." (that never happens) Because I kept hearing the same questions from physicians who were considering opening a practice, I recently created a small physician cohort called Independent Practice Path. It’s an 8-week program focused on helping physicians move from thinking about opening a Direct Care practice to actively preparing to launch. We focus on things like: • mindset shifts involved in moving from employed physician to owner • learning how to explain the DPC model clearly • where and how to start conversations with potential patients • building early interest in the community • putting basic communication and nurture systems in place • collecting a waitlist of interested patients well before opening day The next cohort starts March 24. If anyone here is considering opening a DPC practice in the next 3-9 months and is curious about it, message me or go to the link here: https://ipp.harmonyopshealth.com/
0
0
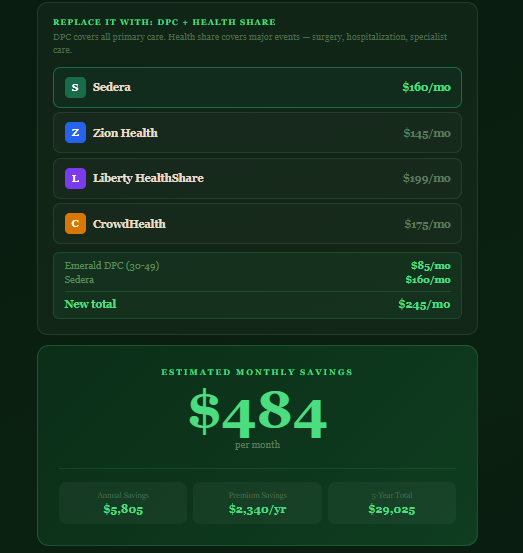
Mar 4 •
Show patients the value of DPC
I built this app in 20 minutes--it's amazing what we can do now! The point of this is to show potential patients the amount of money that they could save with DPC combined with Health Share compared to insurance. Some people need to see it to believe it. https://24-7-bot.harmonyopsfordpc.com/savings
Mar 3 •
DPC Books
People just starting their DPC journey often ask me for good DPC book recommendations. A few of my favorites are Doug Farrago's books, Julie Gunther's Sparks Start Fires, and Paul Thomas' Startup DPC. I also recommend several business books, too. Dr. Una -EntreMD, Megan DiPietro -She Sells, many others. I've listed them here, along with recommendations for other DPC resources and tech. https://24-7-bot.harmonyopsfordpc.com/dpc-resources Do you have any other great book recommendations for beginning DPC?
2
0
1-9 of 9

@anne-gonzalez-6240
I help women feel more like themselves through their perimenopause journey with education, hormones and aesthetic treatments
Active 19d ago
Joined Dec 21, 2025
Powered by