
Write something
Jan 30 •
Broken Bones, and what you need to know!
Framework: MARCH → then Secondary Injury Management 🩸 M — Massive Hemorrhage (FIRST, ALWAYS) Fractures love to bleed—especially femur, pelvis, open fractures. - Look for life-threatening bleeding - Apply: Tourniquet (high & tight if needed) Pressure dressing Wound packing if open + bleeding - Do not splint before bleeding is controlled 👉 Remember: A broken bone can kill via blood loss. 🫁 A / R — Airway & Respiration Usually intact with isolated fractures, but: - High-energy trauma = reassess - Rib fractures? Watch for: Shallow breathing Increasing pain Signs of pneumothorax 🩸 C — Circulation / Shock Fractures can cause internal bleeding. - Check: Skin (cool, pale, clammy) Mental status Radial pulse - Treat for shock: Lay flat (if safe) Keep warm Control pain if within scope 🧠 H — Hypothermia / Head Injury - Exposed patients lose heat fast - Use: Emergency blanket Jackets / vehicle heat - Head injury + fracture = higher priority 🦴 FRACTURE IDENTIFICATION Suspect a fracture if you see: - Deformity or unnatural angle - Swelling / bruising - Pain with movement - Loss of function - Bone visible = open fracture (medical emergency) ⚠️ If it looks broken, treat it as broken. 🔒 SPLINTING: THE GOLD STANDARD Rule: Immobilize the injury and the joints above and below Steps: 1. Expose the injury 2. Check CSM (Circulation, Sensation, Movement) 3. Realign only if needed to restore circulation (and trained to do so) 4. Pad generously 5. Splint & secure 6. Recheck CSM 🧠 Field-expedient splints: - Rifles (safe & unloaded) - Tourniquet windlass rods - Sticks / trekking poles - Cardboard / magazines - SAM splint = king 👑 🚫 WHAT NOT TO DO - ❌ Don’t ignore bleeding - ❌ Don’t force realignment unless circulation is compromised - ❌ Don’t leave jewelry on (swelling risk) - ❌ Don’t forget reassessment 🎯 SCENARIO (Think It Through) You respond to a vehicle vs pedestrian. Patient has: - Obvious lower leg deformity - Bleeding controlled with pressure - Complains of severe pain
1
0

Jan 27 •
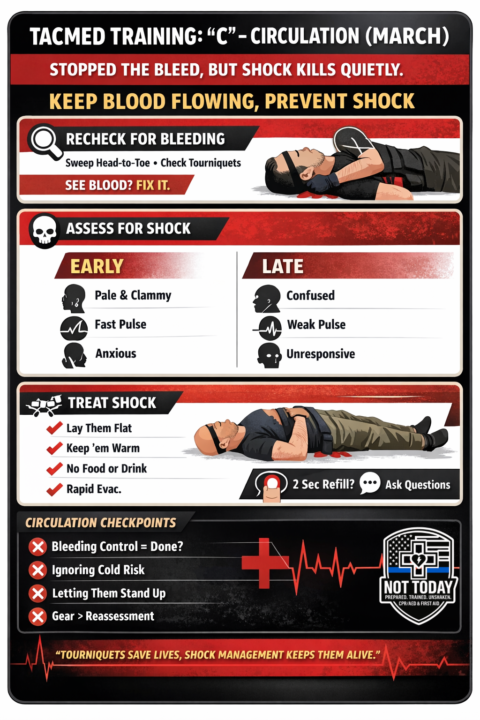
TACMED TRAINING: “C” – Circulation (MARCH)
Why “C” Matters You can stop the bleeding and manage airway/breathing—but if circulation fails, shock kills quietly. “C” is about keeping blood moving, organs perfused, and preventing preventable death. What “C” Covers (Plain Language) Circulation focuses on: - Identifying shock - Managing bleeding you may have missed - Supporting blood flow until higher care arrives Think: “Is blood moving where it needs to go?” Step-by-Step: Circulation Check 1️⃣ Recheck for Bleeding (You WILL miss things) - Quickly sweep head-to-toe - Look under clothing, behind legs, armpits, groin - Check tourniquets: Still tight? Bleeding stopped? Time noted? 👉 Rule: If you see blood, fix it before moving on. 2️⃣ Assess for Shock (This Is the Silent Killer) Early signs: - Pale, cool, clammy skin - Fast pulse - Anxiety, restlessness - Thirst Late signs (bad): - Confusion - Weak or absent pulse - Loss of consciousness 👉 You don’t need a BP cuff—use your eyes and hands. 3️⃣ Treat Shock (Simple, Effective Actions) - Lay them flat (if no contraindication) - Keep them warm (blanket, jacket, space blanket) - Control pain & anxiety (calm voice matters) - Do NOT give food or drink - Rapid evacuation / EMS activation 🧠 Cold + blood loss = clot failure. 4️⃣ Capillary Refill & Mental Status (Quick Field Checks) - Press fingernail → refill >2 seconds = poor perfusion - Ask simple questions: “What’s your name?” “Where are we?” “What happened?” Changes = worsening circulation. Common Mistakes to Avoid 🚫 - ❌ Assuming bleeding control = circulation handled - ❌ Ignoring temperature management - ❌ Letting patients sit or walk unnecessarily - ❌ Focusing on gear instead of reassessment Real-World Mindset Shift: Tourniquets save lives—but shock management keeps them alive long enough to matter. Circulation isn’t flashy. It’s discipline, reassessment, and calm control.
1
0
Jan 23 •
MARCH Breakdown – R = RESPIRATION 🫁
Once massive bleeding is controlled, air in and out matters—now. Respiration focuses on life-threatening chest injuries that prevent effective breathing. 🔍 What you’re looking for: - Penetrating chest wounds (front or back) - Sucking chest wounds - Unequal chest rise - Rapid, labored, or shallow breathing - Chest pain or worsening respiratory distress 🛠️ Immediate actions: - Seal open chest wounds with a vented chest seal(If unvented: burp it if breathing worsens) - Expose and check the back—missed exit wounds kill - Monitor breathing continuously - Be alert for tension pneumothorax signs: Increasing difficulty breathing Anxiety / restlessness Diminished breath sounds on one side Worsening despite treatment - 🧠 Mindset shift: Respiratory problems can deteriorate fast. A patient who’s “okay right now” may not stay that way.
1
0

Jan 13 •
M.A.R.C.H. - AIRWAY
A: Airway Why it matters: No airway = no oxygen = no life. What to Look For - Snoring, gurgling, choking - Blood, vomit, broken teeth - Inability to speak clearly What to Do 1. Position patient 2. Jaw thrust / head tilt–chin lift 3. Clear visible obstructions 4. NPA / OPA as appropriate (if trained) Tactical Considerations - Facial trauma = airway risk - Secure airway without losing scene awareness Note: Most airway failures are positioning failures.
Jan 8 •
Massive Hemorrhage – Reassessment Matters
MARCH: Massive Hemorrhage – Reassessment Matters 🔴 Scenario You arrive first on scene of a vehicle vs pedestrian crash. A bystander applied a tourniquet to the patient’s left thigh. EMS is 6–8 minutes out. The patient is conscious, pale, and anxious. M – Massive Hemorrhage ✅ What To Do - Reassess the tourniquet Is it high and tight? Is bleeding fully controlled? - If bleeding continues: Tighten the tourniquet until bleeding stops Apply a second tourniquet above the first if needed - Check for hidden bleeding Groin, buttocks, armpits, behind knees - If a tourniquet can’t be placed: Pack the wound and apply direct pressure 👀 What To Look For - Blood soaking through clothing or bandages - Pooling blood beneath the patient - Pale or clammy skin - Fast pulse or increasing anxiety (early shock signs) 🆚 Civilian vs Law Enforcement Response 🧍♂️Civilian Focus - Prioritize personal safety - Call 911 early - Use commercial or improvised tourniquets - Apply direct pressure if unsure - Reassess only if safe to do so Goal: Stop the bleeding until help arrives Law Enforcement / First Responder Focus - Ensure scene security - Apply rapid hemorrhage control - Carry and use department-issued TQs and hemostatic gauze - Perform systematic MARCH reassessments - Prepare for handoff to EMS Goal: Stabilize, reassess, and maintain control until transport 👨🏫 Instructor Note Tourniquets fail more often from poor placement or hesitation than from overuse. Pain is expected. Bleeding control always comes first. Reassess after movement, stress, or time passes. 🔑 Key Takeaway The first tourniquet isn’t the finish line — reassessment saves lives.
1-7 of 7
powered by

skool.com/not-today-cpr-and-first-aid-3903
Be ready when it matters. Real-world CPR, First Aid & Stop the Bleed training by a first responder, for families, schools, and first responders.
Suggested communities
Powered by