Activity
Mon
Wed
Fri
Sun
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
What is this?
Less
More
Memberships
Chlorine Dioxide Testimonies
607 members • Free
AI Business Trailblazers Hive
15.2k members • Free
WavyWorld
50.4k members • Free
Cancer Warriors Vault
45 members • $10/month
KetoforCancer
653 members • $9/m
Cancer Warriors
549 members • Free
209 contributions to Cancer Warriors

18d •
Does Anyone Have Experience Using This Natural Compound?
Dr Paul Marik: Modified Citrus Pectin (MCP) binds to a specific protein called Galectin-3. Galectin-3 is expressed on cancer cells and allows them to bind to the endothelium. It allows the cancer cells to get through the endothelium. It allows the cancer cells to clump together, and so it plays a really important role in the metastatic process. There's really good data, particularly in experimental models. If you give MCP, which binds to Galectin 3 you reduce the risk of metastasis. MCP is taken orally. It's safe and has no side effects. EOM -------------------------------------- If so, please share your experience here. Thank you. The video: https://youtu.be/Al_NPY5AiI8?t=2023
2 likes • 17d
@Lisa Drake Nice, thanks for the info! I’m taking the MCP powder and mixing it with warm water first. I stir it well, but it still clumps. I was told the best way to take it without clumping is for maximum absorption. How do you usually take it?

29d •
Pray4Isla
Joining this community to feel less alone as we walk through DIPG with our 12-year-old daughter Isla. Please keep her in your prayers. ❤️
1 like • 21d
@Mili Kader Praying for Isla. That smile of hers is pure light

27d •
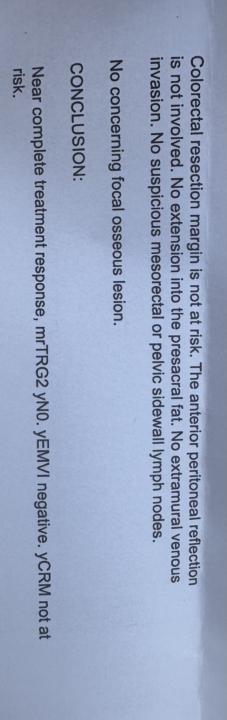
MRI results - near complete response
Hi fellow warriors! ✨ Just a quick update on my journey. I took an integrative approach to my last protocol, combining radiation with fasting, HBOT, repurposed drugs, RLT, and a GKI-friendly meals. I’m happy to share that I’ve achieved a “near complete” treatment response. This result surprised my oncology team, especially since I opted out of standard “Total Neoadjuvant Therapy” (avoiding Oxaliplatin). Because there’s still some scar tissue and inflammation, I’ll need a sigmoidoscopy to see how much of Shrimpy Boy is actually left (if any). My radiation oncologist and I are hoping it’s actually inflammation of surrounding tissues. 🤞 Now I’m moving into a “watch and wait” phase, supported by my oncologist’s knowledge that radiation’s impact can continue to work on tumour cells for months, especially when supported by metabolic therapy. I’m staying patient and vigilant, hoping that this is either a full response or one that will become “complete” very soon. Part of me just wants to fast the shit out anything left, but with knowledge that autophagy can also be weaponised by cancer cells, I’ve decided against this. Best of all I’ve avoided the “near certain” side effects of pelvic radiation—no burns, no bowel issues, and my fertility is intact. I know this might not last forever and I’d be delusionally optimistic to not expect late-onset side side effects. I’m not sure how much longer I’ll stay away from antioxidants due to the “antioxidant paradox”, which ultimately led to my decision to pause some of my supplements and not take Vitamins C, A, E, and CoQ10 during the seven weeks of radiation. Because they act as free-radical scavengers, reintroducing them can risk lowering ROS within the cancer cells, inadvertently shielding Shrimpy Boy from continuous DNA damage over time. I acknowledge that not everyone agrees with pausing antioxidants and that the data remains highly conflicting. Ultimately, this was a decision made strictly for my own peace of mind, rather than an assertion of personal expertise (and is NOT medical advice).
3 likes • 22d
@Lisa Drake What an incredible news! "Near complete" is not just a clinical term, it's a triumph. It's a testament to the countless difficult decisions, the moments of doubt overcome by hope. Wishing you continued healing

Jun 15 •
❤️ It’s Been A While… How Is Everyone Doing?
Hi Warriors ❤️ It’s been quite a while since I’ve posted, and I wanted to check in with everyone. As many of you know, I’ve been going through an incredibly difficult time following the loss of my mum. She was my best friend and the inspiration behind this community. I’ve needed some time to process everything and focus on my family. There are still many unanswered questions surrounding her final hospital admission. I’ve requested access to her medical records and am currently waiting for them. Unfortunately, progress has been slow, and it feels as though things became more defensive once concerns about potential clinical negligence were raised. At the moment, I’m trying to understand exactly what happened. There are several aspects of her care that I still struggle to reconcile, including concerns about severe COVID pneumonitis that appeared to be dismissed, decisions made during her admission, and the rapid decline that followed. My hope is that obtaining the records will provide some clarity and answers. Sometimes I find myself wondering “what if?” and wishing we had been given more time. Everything happened so quickly, and we never even had the opportunity to try the new protocol from Astron Health that we had been exploring. Since losing my mum, I’ve found myself replaying everything over and over in my head. Wondering if there was something else I could have tried, another question I could have asked, another avenue I could have explored. But if I’m completely honest, my biggest regret isn’t a treatment, a protocol, or a therapy that we didn’t try. My biggest regret is not showing her more love. I was so focused on finding answers. So focused on finding a cure so that she could live. I spent countless hours researching, reading studies, analysing scans, tracking symptoms, and learning everything I possibly could. Every day felt like a race against time. I was constantly thinking about the next step, the next blood test, the next scan, the next treatment, the next possibility.
0 likes • Jun 20
@Bernardo Henriques Thank you for sharing your journey, your story inspires me, and your dedication to supporting others in this community is admirable. To answer your question about how I'm doing: I'm doing alright, better than I was when I first joined this community back in 2024. I will share my full story when time permits. For now, I want to shift the spotlight to the heroes who have indirectly transformed my health along the way. They are: 1. Prof Thomas Seyfried 2. Dr. Pierre Kory 3. Dr. Andreas Kalcker 4. Dr. Zsófia Clemens 5. Dr Jack Kruse 6. Dr. Eric Berg 7. Dr. Laurent Schwartz 8. The late Stuart Briscoe
1 like • Jun 23
@Bernardo Henriques Couldn't agree more. Stuart opened my eyes to the power of sunrise and introduced me to the work of Dr. Jack Kruse. Before him, I was completely in the dark about the health benefits of sunrise. I've since turned my life around: I'm now an early bird, rising before dawn to catch those healing natural red light. For those interested in Dr. Kruse, many on YouTube, and I like this one: https://youtu.be/5W6x7EsE8C4?si=x5grZoYPkUIAbP1c
Jun 14 •
Support New Standard Cancer Treatment Options
If you or someone you love is new to a cancer diagnosis, it can be heartbreaking. Unfortunately, you’re not alone, either. The American Cancer Society estimates there are 5000+ cancer diagnoses daily. Regardless of your journey ahead, the key is finding your strength to stay positive and plan ahead. As you begin your search online for resources and hope, you’ll find a lot of the same, prepare for chemotherapy, radiation, surgery, and not feeling well as you endure all of the above. What you won’t find in abundance are resources about how to stay healthy during your cancer fight, using metabolic therapies and proper nutrition. Our goal is clear and ambitious: to gather 1 million signatures from individuals who stand with us in advocating for comprehensive cancer care that includes metabolic therapies and nutrition. By signing our declaration, you’re not just adding a number; you’re raising your voice for a cause that demands attention and action. You’re supporting a movement that empowers every cancer patient with the knowledge and freedom to choose a treatment plan that goes beyond conventional methods. By Healing Humanity Sign the declaration here: https://healinghumanity.movie/sign
1-10 of 209

@fitch-t-8478
I've faced past storms, unsure if I'd escape.
Yet, here I stand.
Facing another storm, unsure if I’d escape.
But I believe I'll escape once more
Active 7d ago
Joined Dec 9, 2024
Indonesia
Powered by